When Pain Needs Permission: The Quiet Reality of Medical Misogyny
A viral post about a woman with endometriosis who needed a man to advocate for her in the ER opens a conversation about medical misogyny, what it is, what the data says, and whether healthcare has a structural problem with women's pain.

A post shared on X recently stopped many people mid-scroll, including me, because it fell on the side of conversations that rarely makes it to the headlines or are fully talked about.
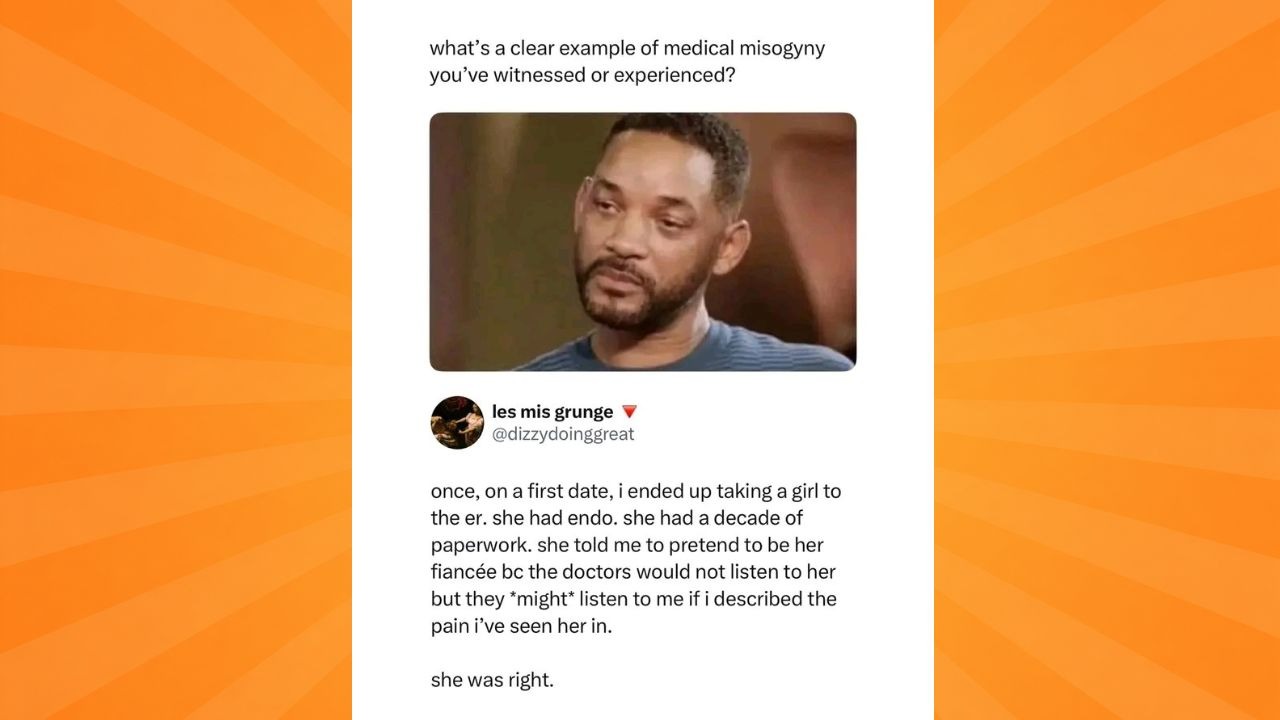
A man described taking a woman he had just met, on a first date, which later ended up to the emergency room in the hospital. She had endometriosis and ten years of medical paperwork documenting her condition, a decade of explaining and experiencing her pain. And still, it wasn’t enough. .
And before they walked in, she made an unsual request: that was pretending to be her fiancé. Not because she wanted the performance or was soliciting for emotional support. Because she knew, from a decade of experience, that the doctors would not take her seriously on her own. But they might listen to him.
She was right. Two words that should not carry as much weight as they do. Two words that confirm what women have been saying about healthcare for a very long time, that the system does not always see them as reliable narrators of their own pain.
That the presence of a man, even a stranger, can change how a medical professional responds to a woman in crisis. That a decade of documented suffering is sometimes less convincing than a man standing next to her saying he has seen what she goes through.
That post is the starting point for a much longer conversation. One about medical misogyny, what it is, what it looks like in practice, what the data says, and whether the healthcare system has a structural problem with women's pain that goes beyond individual “bad“ doctors.
What Medical Misogyny Actually Means and Why Endometriosis Is Its Most Documented Case Study
Medical misogyny refers to the systemic bias within healthcare that results in women's symptoms being dismissed, minimised, or misattributed, particularly when those symptoms involve pain.
It is not always deliberate and does not require a doctor who actively dislikes women. It can operate through training gaps, cultural assumptions, unconscious bias, and a research ecosystem that has historically studied male bodies as the default and treated female physiology as a variation.
Endometriosis, the condition the woman in that post has been living with, is one of the clearest examples of how this plays out at scale.
Endometriosis is a chronic disease in which tissue similar to the lining of the uterus grows outside it, causing debilitating pain, menstrual disruption, fertility complications, and a daily quality-of-life impact that most people who do not have it significantly underestimate. It affects roughly one in ten women globally.
According to research published across multiple peer-reviewed journals in 2025, the diagnostic delay for endometriosis remains between five and twelve years from the onset of symptoms in the developed world. Five to twelve years! for a condition affecting that many people.
The Lancet's obstetrics and women's health journal reported in November 2025 that in a survey of 5,100 women in the United Kingdom, more than half felt their pain had been dismissed or ignored by medical professionals.
The Women and Equalities Committee, in a formal parliamentary report, found that women with endometriosis, adenomyosis, and heavy menstrual bleeding were routinely told their symptoms were normal and their suffering was disregarded.
The American Medical Association's Journal of Ethics noted in 2025 that gender bias renders women more likely than men to have their pain dismissed as psychological by clinicians and that Black women face this implicit bias at even higher rates.
These are not fringe findings from advocacy groups. They are peer-reviewed, parliamentary, and institutional. The data on medical misogyny is not thin. It is stacking up and the woman on that first date had ten years of personal documentation to add to it.
A Decade of Paperwork Was Not Enough. A Man's Voice Was.

Go back to the image containing the X post, she had a decade of paperwork. That is ten years of appointments, diagnoses, test results, treatment records, and documented pain. She walked into that emergency room not as an anonymous patient presenting with vague complaints, but as someone with an extensive medical history that should have spoken for itself.
And yet her first instinct, drawn from ten years of navigating that system, was not to trust that the paperwork would be enough. Her strategy was to bring a man and have him describe what he had witnessed.
The comments under that post filled in quickly. Women sharing their own versions of the same story. Being told their pain was stress. Being prescribed antidepressants when they came in with physical symptoms. Being sent home from emergency rooms in active crisis.
Being told that painful periods were normal, that their threshold for pain was low, that they were being dramatic. The recurring thread here: the experience of being believed faster and more completely when a male partner, family member, or friend was present to corroborate what they were saying. As if a woman's account of her own body required external verification.

A study found that 47% of women with endometriosis had seen at least five different doctors before receiving an accurate diagnosis or referral. Another found that patients who experienced dismissal from medical practitioners had a diagnostic delay of nine years on average, compared to 4.6 years for those who were not dismissed.
The act of not being believed does not just cause emotional distress, it delays treatment, leads to more complications, worsens outcomes, and in some cases causes irreversible damage.
So Is the Healthcare System Designed Against Women or Is That Too Strong a Conclusion?

Here is the honest question. Is this a case of individual doctors making individual mistakes? Or is there something structural, embedded in how medicine has historically been practised, researched, and taught, that produces these outcomes consistently across different countries, different healthcare systems, and different generations of patients?
The evidence points toward the latter. Medical research for decades used male bodies as the standard study subject, with female physiology treated as a hormonal complication rather than a distinct area of study.
Conditions that predominantly affect women have been historically underfunded relative to their prevalence. The very language used to describe women's pain in clinical settings has carried assumptions — hysterical, anxious, dramatic — that shaped how practitioners were trained to respond.
A study found that women were significantly less likely than men to be treated as emergency cases when presenting with chest pain, one of the most serious presenting symptoms in any clinical environment.
So what does it say that a woman with ten years of documented endometriosis history needed to coach a man she had just met to advocate on her behalf in an emergency room?
It says that she had learned, through a decade of experience, that the system's response to her pain was conditional. That her credibility as a patient was not self-sufficient. That the architecture of the room she was entering was not built with her in mind.
Medical misogyny is not a conspiracy theory or an attack. It is a documented, data-supported, institutionally acknowledged pattern of harm.
And until healthcare systems, in their funding, their training, their research priorities, and their clinical culture, reckon seriously with that pattern, women will keep walking into emergency rooms with decades of paperwork and a strategy.
Because they already know what happens when they walk in alone.