BMC Pregnancy and Childbirth volume 25, Article number: 494 (2025) Cite this article
Congenital birth defects (CBDs) rank among the top five causes of death in children under the age of five. Despite their significant impact, studies on the burden of CBDs in G20 countries remain limited. This study sought to examine the temporal trends in the disease burden and mortality rates of CBDs across G20 countries from 1990 to 2021, identify potential risk factors contributing to these trends, and project the disease burden and mortality rates for the period 2022–2040.
Data for this study were obtained from the Global Burden of Disease (GBD) 2021 and GBD 2019 databases. We analyzed trends in disability-adjusted life years (DALYs) and mortality rates for CBDs in G20 countries using absolute numbers, all-age rates, age-standardized rates (ASR), annual percent change (APC), and average annual percent change (AAPC). Joinpoint regression analysis was conducted to identify significant periods of change in ASR. Spearman correlation analysis with locally weighted regression, supplemented by 10,000 bootstrap iterations for robustness validation was used to examine the associations between the socio-demographic index (SDI), healthcare access and quality (HAQ) index, Summary exposure value (SEV) of risk factor exposure, and ASR. Decomposition analysis was performed to investigate the driving factors behind changes in CBDs. Finally, a Bayesian age-period-cohort (BAPC) model was applied to project DALYs and mortality rates for the period 2022–2040.
From 1990 to 2021, the total DALYs and the number of deaths in G20 countries decreased by 59.77% (95% UI: 68.14–35.22%) and 63.81% (95% UI: 38.72–71.64%), respectively, with a more pronounced reduction observed in males compared to females. In 2021, India recorded the highest DALYs and deaths, followed by China and Indonesia. Mexico reported the highest age-standardized DALY rate (ASDR) and age-standardized mortality rate (ASMR), followed by Turkey, with Argentina ranking third for ASDR and Brazil third for ASMR. Congenital heart anomalies (CHAs) remained the leading cause of ASDR and ASMR among CBDs in 2021, with digestive congenital anomalies (DCAs) ranking second. Joinpoint regression analysis indicated that the most significant changes in ASDR in G20 countries occurred between 1995 and 2021 (APC = -2.58, 95% CI: -2.61 to -2.55), while the most pronounced changes in ASMR were observed between 2019 and 2021 (APC = -3.75, 95% CI: -4.75 to -2.86). The periods of significant change in ASR varied across countries. Spearman correlation analysis revealed that countries with higher SDI and HAQ index exhibited lower ASR (p < 0.01, 95% BCa CI excluded zero). Eleven level-3 risk factors showed a positive correlation with ASDR (p < 0.05, 95% BCa CI excluded zero), with the highest absolute correlation coefficients observed for occupational noise, unsafe sanitation, and vitamin A deficiency. Decomposition analysis showed that changes in aging and epidemiological patterns contributed to reductions of -26.19% and − 54.21% in DALYs, respectively, while population growth led to a 20.64% increase in DALYs. The driving factors for DALY changes varied across countries. The BAPC model predicted a declining trend in DALYs, deaths, and ASR of CBDs across all G20 countries in the future.
Although the burden of CBDs has declined in G20 countries, significant disparities persist between nations. To effectively reduce these gaps, enhanced international cooperation, increased investment in healthcare resources, and the implementation of more robust preventive measures are essential to effectively reduce the gap in the CBD burden across these countries.
Congenital birth defects (CBDs), also known as congenital anomalies or birth defects, are structural, functional, or metabolic abnormalities that arise during fetal development in the womb. These abnormalities may be detected prenatally, at birth, or later during infancy. While both genetic and environmental factors are known to contribute to CBDs, the specific causes of many cases remain unclear [1].Current estimates suggest that approximately 240,000 newborns die within the first 28 days of life each year due to congenital diseases, with an additional 170,000 deaths occurring among children between 1 month and 5 years of age [2].Globally, life expectancy and the age-standardized disease burden are projected to improve between 2022 and 2050, with a significant shift in the disease burden from communicable, maternal, neonatal, and nutritional diseases (CMNN) to non-communicable diseases (NCDs) [3].As a subset of NCDs, CBDs were identified as one of the top five causes of death in children under five years old, according to the 2019 Global Burden of Disease (GBD) study [4].Furthermore, as neonatal and under-five mortality rates continue to decline, the proportion of deaths attributable to congenital diseases within these age groups has increased [2].In 2021, the global total fertility rate (TFR) was less than half of what it was in 1950, decreasing from 4.84 (95% UI: 4.63 to 5.06) to 2.23 (95% UI: 2.09 to 2.38). Despite this decline, the annual number of live births exhibited an upward trend, peaking at 142 million (95% UI: 137 to 147 million) in 2016 before declining to 129 million (95% UI: 121 to 138 million) in 2021 [5].The increasing live birth rate, particularly in resource-limited regions, poses significant challenges to healthcare systems, potentially hindering the implementation of effective screening and intervention measures for congenital defects.
Research conducted by the World Health Organization (WHO) indicates that nine out of ten children born with severe congenital diseases originate from low- and middle-income countries [2].Over the past three decades, the global burden of CBDs has generally declined. However, substantial disparities in CBD-related mortality and DALY rates persist across countries and regions. Notably, nations with a low socio-demographic index (SDI) continue to bear a disproportionately high burden of these conditions [6, 7].Between 1990 and 2019, deaths attributable to CBDs in low-SDI regions increased by 14.49%, while other SDI regions experienced reductions exceeding 30% [8].The trends in disease burden also vary by the type of CBD. For instance, in 2017, an estimated 261,247 deaths worldwide were attributed to congenital heart disease (CHD), representing a 34.50% decrease compared to 1990. During the same period, the global mortality rate among infants under one-year-old due to CHD declined by 39.70% [9].Furthermore, from 1990 to 2019, the global prevalence and DALY rates for conditions such as Klinefelter syndrome (KS) and Turner syndrome (TS) exhibited an overall downward trend, whereas rates for urogenital congenital anomalies (UCAs) increased [10].Low-SDI countries and regions experienced the highest mortality and DALY rates for congenital anomalies of the kidney and urinary tract (CAKUT), while medium-low SDI regions recorded the highest prevalence of CAKUT [11].To effectively address the evolving global burden of CBDs, it is imperative to implement more precise and targeted strategies tailored to the specific needs of different regions and populations.
The G20 nations represent the majority of the world’s largest economies and are home to two-thirds of the global population. These countries exhibit significant diversity in terms of geography, economic development, healthcare systems, and medical resources [12].Every year, nearly two million preventable deaths—including stillbirths—occur among mothers, newborns, children, and adolescents within G20 countries [13].While the G20 holds a unique position to lead efforts in tackling critical issues such as environmental pollution, mental health, and maternal and child health, their approaches often diverge from those of other economic organizations [14].Moreover, these countries frequently fall short in prioritizing health equity and lack effective collaboration and coordination to tackle public health challenges [15].Greater and more substantive actions are urgently needed to strengthen cooperation among G20 nations and collectively address the health and well-being challenges faced by women, children, and adolescents. To date, limited research has focused on the long-term trends in the burden of CBDs and their associated risk factors within G20 countries.
In recent years, studies [16, 17] on the disease burden of CBDs have primarily focused on global patterns and regional variations across different socioeconomic development levels (stratified by quintile SDI). Methodologically, these investigations have employed Joinpoint regression analysis, health inequality assessment, decomposition techniques, frontier approaches, and diverse predictive models to systematically evaluate temporal trends and project future trajectories of various CBD subtypes. Notably, the 18th G20 Summit in 2024 (https://g20.org/summit-and-logos/2024-brazil/) explicitly prioritized enhancing healthcare accessibility as a key agenda item. However, two critical knowledge gaps persist in current research: (1) limited exploration of the mechanisms through which national Healthcare Access and Quality (HAQ) indices influence CBD burden, and (2) insufficient multinational comparative analyses examining associations between summary exposure values (SEVs) of risk factors and CBD burden.
To address these gaps, this study innovatively synthesizes data on DALYs and mortality attributed to CBDs across G20 nations from 1990 to 2021. By incorporating country-level SDI, HAQ index, and SEVs of major risk factors, we establish a multidimensional analytical framework. Beyond extending conventional temporal trend analyses, our research specifically investigates: (1) heterogeneous patterns of CBDs burden among G20 countries, and (2) key drivers underlying disease burden evolution in high-burden nations. The findings are expected to provide evidence-based strategies for G20 member states to develop targeted CBDs prevention and control measures, ultimately contributing to sustainable global reduction of birth defect burden.
All data in this study were obtained from the GBD 2021 Results Tool on the Institute for Health Metrics and Evaluation (IHME) website (http://ghdx.healthdata.org/). The GBD 2021 database provides comprehensive estimates for 371 diseases and injuries across 204 countries and territories [18] and epidemiological estimates for 88 risk factors with their attributable health outcomes [19].Data were derived from vital registration systems, verbal autopsies, censuses, household surveys, disease-specific registries, health service utilization records, and other sources [18].GBD 2021 incorporated comprehensive data harmonization procedures to address systematic biases originating from heterogeneous data sources, varying case definitions, and differential measurement methodologies. This analytical framework employed advanced statistical modeling techniques, notably the Meta-Regression-Bayesian, Regularized, Trimmed (MR-BRT) approach and DisMod-MR 2.1 disease modeling software, to establish cross-population comparability across spatial, demographic, and temporal dimensions. Through iterative standardization and empirical calibration algorithms, the methodology effectively reduced measurement heterogeneity and enhanced the validity of comparative risk assessments. For this study, we extracted and analyzed data on trends in DALYs and mortality rates for CBDs in G20 countries from 1990 to 2021, along with their potential influencing factors. The G20 is an international forum comprising 19 countries (Argentina, Australia, Brazil, Canada, China, France, Germany, India, Indonesia, Italy, Japan, Mexico, the Republic of Korea, the Russian Federation, Saudi Arabia, South Africa, Turkey, the United Kingdom, and the United States) as well as the European Union [20].Notably, this research involved a secondary analysis of the GBD database and did not utilize any original patient data; therefore, ethical approval was not required. Throughout the study, we strictly adhered to data usage agreements, ensuring the anonymity and confidentiality of all data.
In the GBD 2021 study, CBDs were identified using the ICD-10 classification system, encompassing cases coded as G71.2, P96.0, Q00–Q15.9, Q17–Q57, Q63.3, Q64–Q64.19, and Q65–Q99.9. These cases were further categorized into 11 distinct subtypes: neural tube defects, congenital heart anomalies, orofacial clefts, Down syndrome, Turner syndrome, Klinefelter syndrome, other chromosomal abnormalities, congenital musculoskeletal and limb anomalies, urogenital congenital anomalies, digestive congenital anomalies, and other congenital birth defects [21].The complete list of ICD codes used for birth defect case identification is provided in Appendix 1.
The GBD 2021 risk factor analysis estimated the SEV for 88 risk factors across various countries and regions worldwide. The SEV reflects the prevalence of risk-weighted exposure within a population [19].Previous studies have provided detailed classifications and definitions for these 88 risk factors [22].Building on this foundation, the present study focuses on analyzing the relationship between the SEV of 41 Level 3 risk factors and the age-standardized rates (ASRs) of mortality and DALYs in G20 countries for the year 2021.
In our study, SDI data for G20 countries (Supplementary Table S3) were obtained from the GBD 2021 dataset. The SDI is calculated as the geometric mean of three key indicators: the total fertility rate among individuals under 25 years of age, the average years of education for individuals aged 15 and older, and the lag-distributed income (LDI) per capita. Each of these indicators is standardized on a scale of 0 to 1 [23].As a composite measure of developmental status, the SDI exhibits a strong correlation with health outcomes, where higher SDI values indicate more advanced levels of socioeconomic development [24].
In our study, the HAQ index for G20 countries (Supplementary Table S3) was derived from the GBD 2019 dataset. The index is calculated as the arithmetic mean of the mortality-to-incidence ratios (MIRs) for 32 causes of death and the risk-standardized death rates (RSDRs). This metric serves as a comprehensive tool for evaluating the quality and timeliness of healthcare services across different countries and time periods [25].The HAQ index ranges from 0 to 100, with higher values reflecting better quality and accessibility of healthcare resources [26].
The number and rate were used to describe the DALYs and mortality associated with CBDs. ASRs were employed to facilitate comparisons of the CBD burden across G20 countries or regions, with 95% uncertainty intervals (UIs) provided to quantify the uncertainty associated with each metric. The UIs were generated from the 25th and 975th ordered values of 1000 posterior distribution draws, following standard GBD protocols. The modeling approach and estimation process are detailed in previous publications [18, 19], and our analysis builds upon this established methodology. The statistical methods employed in this study included Spearman correlation analysis with locally weighted regression, supplemented by 10,000 bootstrap iterations for robustness validation, Joinpoint regression analysis, decomposition analysis, and the BAPC model, which were used to analyze and project the burden of CBDs in G20 countries from 1990 to 2021. Statistical significance was defined as a p-value of less than 0.05. All statistical analyses and data visualizations were conducted using R software (version 4.3.3).
We conducted a Joinpoint regression analysis using the Joinpoint command-line software integrated with R [27]. This analysis was designed to estimate and compare the annual percent change (APC) and average annual percent change (AAPC) in ASRs of CBDs across G20 countries from 1990 to 2021, aiming to reveal differences in disease burden trends. A log-linear model (ln y = β⋅x + constant) was employed to perform segmented regression of temporal trends in CBD disease burden. The grid search method (GSM) was applied to identify all possible grid points, with the point yielding the minimum mean squared error (MSE) selected as the joinpoint. Monte Carlo permutation tests (with a maximum of five and a minimum of zero joinpoints) were utilized to determine the optimal joinpoint regression model. Using the optimal model, we calculated the APC and AAPC to quantify changes in disease burden rates over the study period [16].The formula for APC is:
$$\:APC=(e^{β}\:\:-1)\times\:100\%$$
Where, β represents the regression coefficient of the log-linear model.
The AAPC was computed as the weighted average of APCs across all segments, with the weights assigned in proportion to the duration of each segment. The AAPC represents the overall trend in the burden of CBD from 1990 to 2021. Specifically, an APC or AAPC < 0 indicates a decreasing trend in disease burden, while an APC or AAPC > 0 signifies an increasing trend.
For all Joinpoint regression outputs– including APC, AAPC, and joinpoint locations– we employed the Empirical Quantile Method (EQM) to estimate confidence intervals. This approach was selected based on its superior statistical properties compared to conventional asymptotic methods, particularly when analyzing complex congenital birth defect trends with potential small-sample fluctuations. The methodology and parameter configuration for Joinpoint regression analysis are detailed on the National Cancer Institute’s Surveillance Research Program website (https://surveillance.cancer.gov/help/joinpoint).
To identify the key drivers behind changes in the number of CBD cases among G20 countries, we assessed the relative contributions of population growth, shifts in age structure, and variations in CBD prevalence. This analysis employed the methodological framework proposed by Das Gupta [28], which leverages algebraic techniques to disentangle and standardize the impact of each factor. By doing so, it provides a clear summary of their respective contributions to the observed changes [29].
We employed the BAPC package in R, which integrates the Integrated Nested Laplace Approximation (INLA) method, to develop BAPC models for predicting the numbers, rates, and age-standardized rates (ASRs) of the disease burden of CBDs in G20 countries from 2022 to 2040 [30].These models are based on the framework of generalized linear models (GLMs) and leverage theoretical relationships between disease burden indicators, age structure, and population size. In the model specification, we employed second-order random walk (RW2) priors to smooth the age, period, and birth cohort effects, thereby effectively capturing underlying temporal patterns. The posterior distributions were estimated using INLA algorithm, which directly approximates the posterior marginal distributions through Laplace approximation and numerical integration techniques. For outcome prediction, we utilized the posterior median as point estimates for counts, age-specific rates and age-standardized rates of DALYs and mortality, while constructing 95% confidence intervals based on the 2.5th and 97.5th percentiles of the posterior distributions to comprehensively assess prediction uncertainty. This methodological approach ensures rigorous statistical inference while maintaining robust predictive performance even under data-sparse condition.Population projections for G20 countries from 2022 to 2040, utilized in this study, were obtained from the GBD 2017 dataset.
In 2021, the total DALYs attributable to CBDs in G20 countries reached 18,249.02 thousand (95% UI: 15,517.85–22,020.93), representing a 59.77% reduction (95% UI: 35.22–68.14%) compared to the 1990 total of 45,358.12 thousand (95% UI: 32,734.57–57,037.52). The burden of disease was notably higher among males (10,047.95 thousand; 95% UI: 8,380.22–12,442.24) compared to females (8,201.06 thousand; 95% UI: 6,838.96–10,316.33). Among G20 countries, India recorded the highest number of DALYs (7,814.43 thousand; 95% UI: 6,037.52–10,361.18), followed by China (3,224.75 thousand; 95% UI: 2,699.60–3,856.10) and Indonesia (1,465.26 thousand; 95% UI: 1,147.04–1,907.56). Conversely, Australia reported the lowest DALYs (51.80 thousand; 95% UI: 45.44–60.57) (Table 1; Fig. 1). The ASDR in G20 countries in 2021 averaged 568.89 (95% UI: 482.58–695.95), representing a substantial decline compared to the 1990 rate of 1,227.68 (95% UI: 884.37–1,544.90). The ASDR was higher among males (605.85; 95% UI: 500.93–763.20) than among females (528.69; 95% UI: 433.91–677.10). At the individual country level, Mexico had the highest ASDR (925.34; 95% UI: 764.98–1,120.51), followed by Turkey (805.41; 95% UI: 662.44–963.03) and Argentina (717.59; 95% UI: 598.32–862.54). The Republic of Korea reported the lowest ASDR (248.70; 95% UI: 200.62–306.58) (Table 1; Fig. 2). India, Mexico, and Brazil consistently ranked high in both total DALYs across all age groups and age-standardized rates, underscoring a significant disease burden in these countries.

Temporal trends in all-age counts of DALYs (A) and deaths (B) attributable to congenital birth defects (CBDs) in G20 nations, India, China, and Indonesia, categorized by sex (1990–2021)
We next analyzed the ASDR for various types of CBDs across different countries and regions (Fig. 3). Between 1990 and 2021, the top five CBDs in G20 countries, excluding “Other congenital birth defects” and “Other chromosomal abnormalities”, were Congenital Heart Anomalies (CHAs), Digestive Congenital Anomalies (DCAs), Congenital Musculoskeletal and Limb Anomalies (CMLAs), Neural Tube Defects (NTDs), and Down Syndrome (DS). While their rankings showed minor fluctuations over time, CHAs consistently held the top position throughout the period, while NTDs fell from third place in 1990 to fifth in 2021. Turner Syndrome and Klinefelter Syndrome consistently ranked last during this period. The rankings for individual countries largely mirrored the overall trends observed in the G20. In most countries, CHAs, DCAs, CMLAs, NTDs, and DS remained the leading CBDs. Notably, in 2021, Saudi Arabia’s ASDR for CHAs ranked second, surpassed only by “Other congenital birth defects”. In France, Italy, and Japan, however, NTDs fell to eighth place in the ASDR rankings.

Comparative analysis of age-standardized DALYs rates (A) and mortality rates (B) for CBDs in G20 countries: 1990 vs. 2021

National rankings of age-standardized DALYs rates for CBDs among G20 members in (A) 1990 and (B) 2021
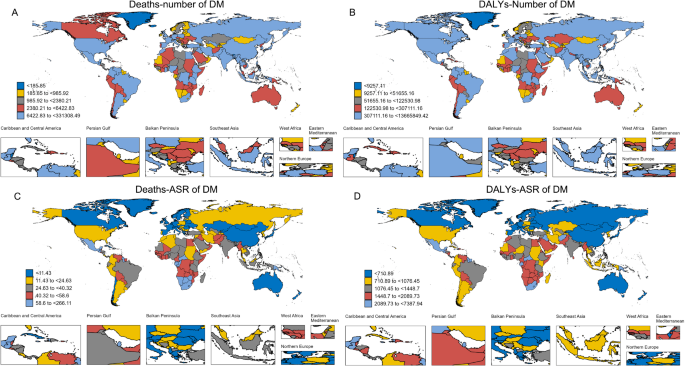
In 2021, the total number of deaths attributed to CBDs in G20 countries was 173,92 thousand (95% UI: 146.61–212.90), representing a 63.81% reduction compared to 1990, when the figure stood at 480.58 thousand (95% UI: 337.04–609.68). Male mortality (96.97 thousand; 95% UI: 79.95–123.17) was significantly higher than female mortality (76.96 thousand; 95% UI: 62.79–100.55). Among G20 countries, India reported the highest number of deaths (74.65 thousand; 95% UI: 56.32–102.94), followed by China (29.15 thousand; 95% UI: 24.00–36.06) and Indonesia (14.36 thousand; 95% UI: 10.61–19.35). In contrast, the Republic of Korea recorded the lowest number of deaths (0.32 thousand; 95% UI: 0.27–0.43) (Table 2; Fig. 1). The age-standardized mortality rate (ASMR) for CBDs in G20 countries was 5.57 per 100,000 population (95% UI: 4.63–6.90) in 2021, marking a significant decline from the 1990 rate of 13.03 (95% UI: 9.13–16.53). The male ASMR (5.98; 95% UI: 4.85–7.75) was slightly higher than that of females (5.12; 95% UI: 4.10–6.80). Mexico had the highest ASMR (9.47; 95% UI: 7.70–11.66), followed by Turkey (8.11; 95% UI: 6.51–9.86) and Brazil (7.17; 95% UI: 5.95–8.59). Conversely, the Republic of Korea reported the lowest ASMR (1.52; 95% UI: 1.20–2.08). Notably, India, Mexico, and Brazil consistently exhibited higher mortality numbers and ASMR compared to other G20 countries (Table 2; Fig. 2).
We subsequently compared the rankings of ASMR for different CBDs across G20 countries in 1990 and 2021. The results (Supplementary Figure S1) indicated that in 1990, CHAs, NTDs, and DCAs were the top three leading causes of mortality. However, by 2021, slight shifts in these rankings were observed: the mortality rate for NTDs decreased to third place, while DCAs rose to second place. Over the same period, the ASMR ranking for DS remained relatively stable, consistently holding the fourth position. Overall, CHAs, NTDs, DCAs, and DS have persistently dominated the ASMR rankings among G20 countries. The most significant changes were observed in the rankings of NTDs experienced a decline in rankings across all countries, whereas UCAs showed varying degrees of increase.
The ASDR for CBDs in G20 countries exhibited an overall declining trend from 1990 to 2021, with an AAPC of -2.44 (95% CI: -2.47 to -2.40; Table 1; Fig. 4). Similarly, the ASMR showed a downward trend, albeit at a slower pace, with an AAPC of -0.19 (95% CI: -0.20 to -0.18; Table 2; Fig. 4). The most pronounced decline in ASDR occurred between 1995 and 2021, with an APC of -2.58 (95% CI: -2.61 to -2.55). In contrast, the most significant reduction in ASMR was observed between 2019 and 2021, with an APC of -3.75 (95% CI: -4.48 to -2.86; Fig. 4). From 1990 to 2021, Saudi Arabia demonstrated the most rapid decline in ASDR (AAPC = -5.22, 95% CI: -5.30 to -5.15), followed by Turkey (AAPC = -4.66, 95% CI: -4.75 to -4.58) and China (AAPC = -4.11, 95% CI: -4.20 to -4.04). Conversely, South Africa showed the slowest decrease (AAPC = -0.71, 95% CI: -0.76 to -0.68). Notably, while ASDR generally declined across all G20 countries during this period, specific intervals experienced slight increases in some nations. For instance, Mexico experienced a marked rise in ASDR from 1990 to 1992 (APC = 1.87, 95% UI: 0.54 to 2.89). Similarly, Saudi Arabia also recorded the steepest reduction in ASMR from 1990 to 2021 (AAPC = -5.61, 95% CI: -5.69 to -5.54), followed by Turkey (AAPC = -4.94, 95% CI: -5.03 to -4.85) and the Republic of Korea (AAPC = -4.81, 95% CI: -4.97 to -4.39). South Africa again showed the slowest decline in ASMR (AAPC = -0.79, 95% CI: -0.85 to -0.74). Interestingly, despite the overall downward trend in ASMR, some countries, including Brazil, Mexico, the Russian Federation, South Africa, and the United Kingdom, experienced minor increases during specific periods. For example, Mexico exhibited the largest rise in ASMR from 1990 to 1992 (APC = 2.20, 95% UI: 0.70 to 3.33). Complete results of the Joinpoint regression analyses are provided in Supplementary Tables S1 and S2.

Longitudinal changes in (A, C) age-standardized DALYs rates and (B, D) mortality rates for CBDs across G20 countries (1990–2021)

Bubble plots visualizing associations of (A) SDI and (B) HAQ index with age-standardized DALYs/mortality rates for CBDs in G20 nations
To assess the impacts of the SDI and HAQ index on the burden and mortality of CBDs, we performed Spearman correlation analyses with locally weighted regression, supplemented by 10,000 bootstrap iterations using data from G20 countries. The analysis included the 2021 SDI, the 2019 HAQ index, and the 2021 ASDR and ASMR. The results revealed a strong negative correlation between SDI and both ASDR (ρ = -0.78, p < 0.01; 95% BCa CI:-0.92, -0.58) and ASMR (ρ = -0.79, p < 0.01; 95% BCa CI:-0.92, -0.58)(Fig. 5; Supplementary Table S7). Countries with higher SDI values generally exhibited lower ASDR and ASMR. However, notable exceptions were observed: Mexico, Argentina, and Turkey had higher ASDR and ASMR compared to other nations with similar SDI levels, whereas China, Italy, and the Republic of Korea demonstrated lower ASDR and ASMR values. Similarly, the HAQ index showed a significant negative correlation with ASDR (ρ = -0.83, p < 0.01; 95% BCa CI:-0.96, -0.66) and ASMR (ρ = -0.82, p < 0.01; 95% BCa CI:-0.94, -0.67) (Fig. 5; Supplementary Table S7). Countries with higher HAQ indices tended to have lower ASDR and ASMR. Among countries with comparable HAQ indices, India, Mexico, Argentina, and Turkey exhibited relatively higher ASDR and ASMR, while Saudi Arabia, the Russian Federation, and the Republic of Korea showed comparatively lower values.
To identify the driving factors behind changes in the burden of major CBDs, we conducted a decomposition analysis of DALYs associated with four primary CBDs—CHAs, DCAs, CMLAs, and NTDs—across G20 countries (Table 3, Supplementary Table S4, Fig. 6). Between 1990 and 2021, the overall DALYs for CBDs in G20 countries decreased by 59.77%. This decline was primarily driven by epidemiological changes, which accounted for a 54.21% reduction, and aging, which contributed to a 26.19% decrease. In contrast, population growth increased the burden by 20.64%. The contributions of these driving factors varied among countries. In most nations, population growth was associated with an increased CBD burden, whereas aging and epidemiological changes contributed to significant reductions. By 2021, the burden of CHAs, DCAs, CMLAs, and NTDs exhibited varying degrees of decline compared to 1990. Aging and epidemiological changes consistently reduced the burden of these conditions across G20 countries. However, population growth was associated with an increased burden for all four major CBDs. Notably, in the Russian Federation, population growth, aging, and epidemiological changes collectively contributed to a reduction in the burden of CBDs. Over the past 32 years, while the overall burden of the four major CBDs has significantly declined at the G20 level—particularly for CHAs, DCAs, and NTDs in most countries—CMLAs exhibited a marked increase in burden in several nations, including Brazil, Canada, Saudi Arabia, Indonesia, Australia, South Africa, and Argentina, which was primarily driven by population growth.

Decomposition of percentage changes in DALYs attributable to four major congenital anomalies among G20 populations (1990–2021): (A) overall CBDs, with subcomponents (B) CHAs, (C) CMLAs, (D) DCAs, and (E) NTDs
To examine the relationship between potential environmental risk factors and the burden of CBDs, we performed a Spearman correlation analysis to assess the association between the SEV of 41 level-3 risk factors in 2021 and the ASDR of CBDs in G20 countries. The analysis identified 13 level-3 risk factors with significant positive correlations to the ASDR of CBDs across countries (p < 0.01). After bootstrap validation (10,000 iterations), eleven risk factors continued to show statistically significant associations with ASDR (Supplementary Table S5). Notably, occupational noise, unsafe sanitation, and vitamin A deficiency emerged as the top three factors with the strongest associations (Supplementary Table S6-7;Figure 7). Specifically, countries such as Mexico, Turkey, and South Africa exhibited higher ASDRs compared to other nations with similar SEVs for occupational noise. In contrast, the Republic of Korea, Australia, and Saudi Arabia demonstrated lower ASDRs under comparable SEVs. Notably, despite China recording the highest SEV for occupational noise, its ASDR for CBDs remained relatively low. In the case of unsafe sanitation, Argentina, Mexico, and Brazil showed elevated ASDRs compared to other countries with similar SEVs, while the Republic of Korea, the Russian Federation, and China exhibited lower ASDRs. India emerged as the country having the highest SEV for unsafe sanitation, which corresponded to a markedly high ASDR for CBDs. Regarding vitamin A deficiency, Mexico, Turkey, and Saudi Arabia experienced higher ASDRs among countries with comparable SEVs, whereas the Republic of Korea and South Africa showed lower ASDRs. It is worth noting that India exhibited the highest SEV for unsafe sanitation, accompanied by a significantly elevated ASDR for CBDs. Conversely, three factors were negatively correlated with the ASDR of CBDs across countries (p < 0.05). After bootstrap validation (10,000 iterations), only two factors - suboptimal breastfeeding and diet high in processed meat - retained significant inverse associations (Supplementary Table S5).

(A) Scatter plots of selected risk factors versus CBDs DALYs rates, with (B) geospatial distribution of three risk factor SEVs (occupational noise, unsafe sanitation, vitamin A deficiency) across G20 countries
Using the BAPC model, we projected the numbers and rates of DALYs and mortality attributable to CBDs across all G20 countries from 2022 to 2040 (Table 4; Fig. 8;Supplementary Table S8; Figure S2). The results indicated an overall decline in both metrics across all countries. India, China, and Indonesia are expected to remain the top three contributors to CBD-related DALYs, while Australia is projected to have the lowest burden. In terms of ASDR, South Africa, India, and Mexico are anticipated to have the highest rates, whereas China and the Republic of Korea are expected to have the lowest. Similarly, India, China, and Indonesia are predicted to account for the highest numbers of CBD-related deaths, with Argentina expected to record the lowest figures. Regarding ASMR, South Africa, India, and Mexico are again expected to rank highest, while the Republic of Korea and China are likely to have the lowest rates. Notably, by 2040, although China is projected to maintain high absolute numbers of DALYs and deaths due to CBDs, significant declines in ASDR and ASMR are expected. In contrast, India presents a more concerning outlook, with persistently high absolute counts of DALYs and deaths, alongside elevated ASDR and ASMR. South Africa and Mexico, despite having lower absolute burdens compared to India and China, are projected to exhibit some of the highest ASRs among the G20 countries.

Sex-stratified trends in case counts and age-standardized DALYs rates for CBDs in G20 countries: observed (1990–2021, solid lines) and BAPC-projected (2022–2040, dashed lines)
Herein, a comprehensive analysis of the burden of CBDs in G20 countries was conducted, encompassing trends over time in DALYs, mortality rates, and their corresponding ASRs, as well as regional and gender disparities. The associations between the burden of CBDs and various determinants, including the SDI, HAQ Index, and environmental risk factors (as measured by SEVs), were investigated. Moreover, the study employed decomposition analysis to identify the driving factors behind changes in the burden of major CBDs, including CHAs, DCAs, CMLAs, and NTDs. Finally, the study projected DALYs and mortality rates for CBDs in G20 countries from 2022 to 2040. These findings underscore the substantial public health challenges posed by CBDs in G20 countries and offer critical insights to inform policy development and optimize resource allocation.
The present study findings revealed that between 1990 and 2021, the total DALYs attributed to CBDs in G20 countries decreased significantly by 60.00%, with a more pronounced decline observed among males. This trend was consistent with findings from global disease burden studies on CBDs [16] and might be attributed to improvements in global healthcare conditions, advancements in medical technology, and the strengthening of preventive measures. However, significant heterogeneity in CBDs burden exists within G20 nations. Despite relatively low prevalence rates, both India and China account for substantial absolute numbers of CBDs-related DALYs and deaths due to their large population bases. Our data show China achieved significantly greater reductions in CBDs burden than India between 1990 and 2021, with lower ASDR and ASMR by 2021. This disparity may be attributed to distinct demographic structures - India’s younger population maintains higher fertility rates that may elevate CBDs burden, while China’s aging population structure, influenced by historical family planning policies, shows different patterns. However, recent policy adjustments and gradually recovering fertility rates in China may lead to increased CBD incidence and mortality, potentially exacerbating the disease burden in coming years. Furthermore, inadequate healthcare resource allocation - including limited medical facilities, insufficient specialized healthcare workers, diagnostic technology gaps, and suboptimal utilization and coverage of prenatal screening and diagnostic measures [31,32,33] - may contribute to delayed detection and treatment of congenital anomalies. Our findings demonstrate strong associations between SDI / HAQ Index and CBDs ASDR/ASMR across G20 countries, providing a plausible explanation for the observed inter-country differences in CBD burden.
The disparities in the burden and mortality rates of CBDs may also be associated with exposure to environmental risk factors [34,35,36,37]. In 2021, countries such as Mexico, Turkey, Brazil, and Argentina exhibited higher ASDR and ASMR, followed closely by India and Indonesia. This study found that these countries had higher SEV for key risk factors. For instance, the top three countries with the highest SEV for occupational noise were China, Indonesia, and Brazil; for unsafe sanitation, they were India, China, and Turkey; and for vitamin A deficiency, they were India, Indonesia, and Brazil. Occupational noise is a significant environmental risk factor. Indeed, prolonged exposure to high-noise environments can lead to hearing loss, cardiovascular diseases, and developmental abnormalities in fetuses. Unsafe sanitation can result in water pollution and the spread of infectious diseases, posing significant health risks to pregnant women and newborns. Poor sanitation increases pregnant women’s exposure to pathogens and harmful substances, thereby elevating the risk of congenital defects. Vitamin A is an essential nutrient for fetal development, and its deficiency can lead to developmental abnormalities and congenital defects [38]. In economically disadvantaged countries, limited public awareness of nutritional supplementation and inadequate provision of vitamin A for pregnant women may adversely affect fetal health.
Among G20 countries, notable gender differences exist in the disease burden of CBDs, with males consistently showing higher DALYs and mortality rates compared to females. This observation aligned with findings from numerous previous studies [32, 39,40,41].These disparities can be attributed to a combination of biological, environmental, and sociobehavioral factors. From a biological perspective, males possess a single X chromosome, whereas females have two. Certain congenital conditions, such as hemophilia and specific types of muscular dystrophy, are caused by mutations on the X chromosome. Since males lack a second X chromosome to compensate for such mutations, they are more likely to experience higher incidence and severity of these conditions. Moreover, genes located on the Y chromosome have been implicated in certain congenital defects, such as Klinefelter syndrome, which predominantly affects males and contributes to their higher DALYs and mortality rates. In some countries and regions, males may also be more likely to seek medical attention, or healthcare systems might prioritize the diagnosis of congenital defects in males, potentially resulting in higher diagnosis and reporting rates. Furthermore, males may have better access to high-quality medical services and treatments in certain contexts, which could influence statistics on DALYs and mortality rates to some extent. Further research is essential to investigate the underlying causes of these gender disparities and to develop targeted prevention and intervention strategies.
Projections for future trends in DALYs and mortality rates associated with CBDs indicate that while most G20 countries are likely to witness a decline in disease burden, India, China, and Indonesia are expected to continue grappling with significantly high levels. These findings underscore the urgent need for targeted public health policies and interventions. Key priorities should focus on advancing socioeconomic development, improving the quality and accessibility of healthcare services, mitigating environmental risks, reducing exposure to harmful environmental factors, and enhancing nutritional standards. Specifically, countries experiencing > 40.00% population growth-associated increases in DALYs (India, Saudi Arabia, and South Africa) should prioritize perinatal healthcare infrastructure development to address the escalating CBD burden. Furthermore, nations with suboptimal healthcare quality (India, Indonesia, and Mexico) must enhance preventive service accessibility, particularly through implementing universal prenatal ultrasound screening programs, to effectively reduce disease burden. Countries with high occupational noise exposure levels (China, Indonesia, and Brazil) require strengthened occupational health regulations to counteract potential CBD burden exacerbation from industrial environmental risks. This study demonstrates a robust association between vitamin A deficiency and CBD burden, prompting our recommendation to integrate routine maternal micronutrient screening (particularly for vitamin A) into prenatal care systems of high-burden nations (India, Indonesia, and Mexico) for targeted primary prevention. Additionally, countries with inadequate WASH (water, sanitation, and hygiene) facilities (India and China) should implement measures to improve both the quality and accessibility of sanitary infrastructure to reduce infection-mediated CBD risks during pregnancy. Such efforts can effectively alleviate the burden of CBDs and help bridge disparities in disease burden across G20 nations. Looking ahead, fostering close collaboration among G20 countries will be critical to achieving improved public health outcomes and enhancing the overall well-being of their populations.
This study has several limitations that warrant consideration. First, in some low- and middle-income countries, the lack of comprehensive health statistics systems may result in incomplete or inconsistent data, potentially leading to an underestimation or inaccuracies in disease burden estimates for these regions. Second, since CBDs predominantly occur during the neonatal period, we were unable to conduct a comparative analysis of disease burden across different age groups. Third, the GBD database does not provide data on the attribution of specific risk factors to the burden of CBDs. Consequently, our analysis was confined to exploring the relationship between the SEV of risk factors and ASR at the national level rather than conducting a detailed assessment of attributable risk factors. Lastly, the absence of comprehensive population projections for G20 countries in the GBD database restricted our ability to predict the burden and mortality rates of CBDs across the G20 nations as a whole.
This study provides a comprehensive analysis of the burden of CBDs in G20 countries. From 1990 to 2021, the DALYs, mortality rates, and ASRs associated with CBDs in these nations showed a declining trend, although significant variations were observed across different countries. Notably, nations with higher SDI and HAQ index scores experienced a lower burden of CBDs and reduced mortality rates. Among the 16 risk factors associated with the ASDR of CBDs, occupational noise, unsafe sanitation, vitamin A deficiency, iron deficiency, and unsafe water sources emerged as the most critical contributors, warranting increased attention. Looking ahead to 2040, the burden of CBDs is projected to decline further. However, reducing disparities in the burden of CBDs requires closer collaboration among G20 countries. Prioritizing investment in healthcare resources, improving accessibility, and implementing widespread preventive measures are essential strategies for effectively reducing the burden of CBDs and achieving more equitable health outcomes across G20 nations.
The data supporting this study are derived from the Global Burden of Disease Study 2021 (GBD 2021), which offers comprehensive estimates of health metrics, including congenital birth defects, across 204 countries and territories. These estimates are publicly accessible through the Global Health Data Exchange (GHDx) at [https://vizhub.healthdata.org/gbd-results/].The datasets generated and/or analysed during the current study are available in the [Global Health Data Exchange GBD Results Tool] repository, [https://vizhub.healthdata.org/gbd-results/].
- AAPC:
-
Average annual percent change
- APC:
-
Annual percent change
- ASDR:
-
Age-standardized DALY rate
- ASMR:
-
Age-standardized mortality rate
- ASR:
-
Age-standardized rate
- BAPC:
-
Bayesian age-period-cohort
- CAKUT:
-
Congenital anomalies of the kidney and urinary tract
- CBDs:
-
Congenital birth defects
- CHAs:
-
Congenital heart anomalies
- CHD:
-
Congenital heart disease
- CMNN:
-
Communicable, maternal, neonatal, and nutritional diseases
- DALYs:
-
Disability-adjusted life years
- DCAs:
-
Digestive congenital anomalies
- EQM:
-
Empirical Quantile Method
- G20:
-
Group of Twenty
- GBD:
-
Global Burden of Disease
- GHDX:
-
Global Health Data Exchange
- GLMs:
-
Generalized linear models
- GSM:
-
Grid search method
- HAQ:
-
Healthcare access and quality
- IHME:
-
Institute for Health Metrics and Evaluation
- INLA:
-
Integrated Nested Laplace Approximation
- KS:
-
Klinefelter syndrome
- LDI:
-
Lag-distributed income
- MIRs:
-
Mortality-to-incidence ratios
- MR-BRT:
-
Meta-Regression-Bayesian, Regularized, Trimmed
- MSE:
-
Mean squared error
- NCDs:
-
Non-communicable diseases
- RSDRs:
-
Risk-standardized death rates
- RW2:
-
Second-order random walk
- SDI:
-
Socio-demographic index
- SEV:
-
Summary exposure value
- TFR:
-
Total fertility rate
- TS:
-
Turner syndrome
- UCAs:
-
Urogenital congenital anomalies
- UIs:
-
Uncertainty intervals
- WHO:
-
World Health Organization
We would like to thank all the participants and contributors to this study.
This study was supported by the Special Research Program of the Education Department of Shaanxi Provincial Government [No. 21JK0600], the Provincial Undergraduate Training Program for Innovation and Entrepreneurship [No.S202410716126], and the Qinchuangyuan Industrial Cluster Zone Joint Fund Project [No.172].
This study is a secondary analysis of publicly available data from the Global Burden of Disease Study 2021 (GBD 2021) database. As the data is anonymized and does not involve direct interaction with human participants, ethical approval and informed consent to participate were not required for this study.
The authors confirm that they have obtained consent for publication from all individuals or entities whose data or images are included in this manuscript. No part of the manuscript has been published elsewhere or is under consideration for publication in any other journal. The authors agree to the publication of this manuscript in the selected journal.
The authors declare no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

Li, X., Qu, P., Yan, P. et al. Trends in burden and mortality of congenital birth defects in G20 countries (1990–2021) and predictions for 2022–2040. BMC Pregnancy Childbirth 25, 494 (2025). https://doi.org/10.1186/s12884-025-07617-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-025-07617-w