Annals of General Psychiatry volume 24, Article number: 22 (2025) Cite this article
Late-life depression (LLD) stands as a prevalent mental health issue among older adults, frequently intertwined with cardiovascular and cerebrovascular diseases as well as cognitive decline. The occurrence of LLD in the older adults, who often present with multiple aging-related conditions, frequently results in this disorder being overlooked. However, the astronomical treatment costs and the considerable societal burden associated with LLD necessitate urgent and sustained attention.
Utilizing data from the Global Burden of Diseases, Injuries, and Risk Factors Study 2021 (GBD 2021), we extracted incidence rates and disability-adjusted life years (DALYs) of LLD in individuals aged 60 and older. The extracted data underwent rigorous evaluation through the application of age-period-cohort models, the health inequality concentration index, and frontier analysis.
From 1990 to 2021, a global increase was observed in both the age-standardized incidence rate (ASIR) and DALY rate of LLD. Specifically, the ASIR ascended by 0.01 per 100,000 annually, while the DALY rate rose by 0.03 per 100,000 each year. Notably, a statistically significant inverse relationship was identified between ASIR and the Socio-demographic Index (SDI) (p < 0.001). Additionally, a notable linear correlation was discerned between age-standardized death rate (ASDR) and SDI, albeit without a discernible downward trend (p < 0.001). According to the SDI, the Estimated average percentage change (EAPC) of five SDI districts showed no increase or decrease. Globally, the incidence of LLD showed an upward trend in the high SDI, middle SDI, and low-middle SDI regions, a downward trend in the high-middle SDI region, and no significant increase or decrease in the low SDI region. In the age-period-cohort analysis, we found that the incidence of LLD increased with age in high and middle SDI regions compared with low SDI regions, and the results were the opposite in low SDI regions, with significant regional characteristics. The period effect analysis revealed that irrespective of gender, the trends in incidence and DALY rates remained relatively unchanged globally from 1992 to 2021. As SDI levels rose, the SDI-adjusted disparities in incidence and DALY rates tended to stabilize. A comparative analysis of data from 1990 to 2021 highlighted a relative decline in health inequalities.
This comprehensive assessment of the disease burden of LLD among the global population aged 60 and older underscores significant accomplishments while simultaneously emphasizing areas requiring ongoing vigilance. In the context of relentless population growth and aging, the favorable downturns in incidence and DALY rates reflect tangible advancements in managing LLD.
Depressive Disorder (DD) is a prevalent mental illness that is typified by a persistently poor mood, lack of enjoyment, or disinterest in activities. Major depressive disorder (MDD) in individuals 60 years of age or more is known as LLD [1]. According to the findings of earlier research, the prevalence of LLD is 28.4%~31.8% worldwide [2,3,4], and it might be higher among those who also have other underlying conditions. About 5% of older people in the community fulfill the DSM5 criteria [3], whereas 10%~16% of older adults patients still exhibit severe clinical symptoms of depression but do not yet meet the diagnostic criteria [4]. LLD is frequently more common in communities and nursing facilities. As a prevalent mental illness among the older adults, LLD is frequently linked to poor outcomes, including death, cardiovascular and cerebrovascular diseases, and cognitive impairment [5,6,7]. It also interferes with the older adults’ normal life, resulting in high medical costs and a significant social burden [8, 9]. Existing evidence fully shows that LLD not only seriously affects the quality of life of the older adults, but also increases mortality and shortens disability-free life [10]. In addition, they increase the risk of falls and are strongly associated with frailty [11]. According to one study, patients with LLD had outpatient healthcare expenses that were 43.0%~52.0% higher than those without LLD, and their combined outpatient and inpatient healthcare costs were 47.0%~51.0% higher [12]. It is important to remember that individuals with LLD frequently experience other aging-related issues. It is important to note that patients with LLD often have other complications related to aging, which increases the complexity of treating LLD with multiple diseases, often with reduced efficacy and increased side effects of antidepressants [13]. The number of older adults people affected by depression will also increase significantly as the population ages to varying degrees around the world. In the United States, LLD is a heavy public health burden for the older adults, and healthcare costs are significantly higher among patients with LLD [14]. LLD is the mental illness with the highest percentage of “disability-adjusted life years” or DALYs, and LLD is associated with increased all-cause mortality: older adults with depression have a 1.65-fold higher risk of death than those without depression, and both severity and duration of depression are associated with excess mortality [14, 15]. For China, which has the largest older adult population in the world, LLD is a major public health problem among the older adults in China. Compared with the young and middle-aged people, depression is more common and serious [16], and it is one of the reasons for the high suicide rate of the older adults in China. Although the incidence of LLD is high and the disease burden is heavy, it has not been paid attention to by the health system departments of various countries and has not been included in the strategic prevention policies of the government. Therefore, LLD is often ignored and not fully treated by patients and medical institutions.
There are currently no reports on the illness burden and epidemiological statistics of LLD worldwide, as well as in other nations and areas. In this field, there is a research gap. However, LLD has raised the burden of sickness among the older adults and placed a certain financial strain on national, regional, and international healthcare systems. In light of this, we think that doing this study is essential.
In order to improve health systems and eradicate disparities, the GBD study is the biggest and most thorough study to date to measure health losses across time periods and locations. The Global Burden of Disease for 2021 measures the burden of 87 hazards, 371 illnesses, and injuries across 204 nations and territories between 1990 and 2021. The prevalence of depression in the older adults is currently the subject of only one age-period-cohort analytic study worldwide [17], and a thorough evaluation of the burden of LLD is either completely unknown or undocumented. From 1990 to 2021, we looked at the prevalence and DALYs of LLD in people aged 60 and over at the national, regional, and worldwide levels based on the older population’s age, sex, and social development level. We also evaluated variables that might affect DALYs in LLD patients.
GBD 2021 is a huge multinational cooperation that covers the global burden of diseases, injuries, and risk factors for 371 diseases in 21 GBD regions and 204 nations and territories from 1990 to 2021. This study uses the LLD data from GBD 2021 for its analysis. is the biggest and most thorough scientific investigation to date that aims to measure health trends and levels [18]. All information is freely available on the GBD website (https://www.healthdata.org/research-analysis/gbd).
Depression in people 60 years of age and older is known as LLD. In addition to lowering the quality of life and social function of older adult patients, it also increases the load on caregivers. It is a frequent mental disorder in the older adult population, and its prevalence may be higher in patients with concurrent physical ailments [19, 20]. During the GBD 2021, we evaluated adults over 60 who had clinically diagnosed depression. According to GBD 2021, depression is a level 4 cause. Since numerous epidemiological data on LLD have not been addressed separately, we did not differentiate between the presence of severe depression and dysthymia in GBD 2021.
The SDI is a comprehensive indicator of social and demographic development. SDI information of each country or region is obtained based on the comprehensive evaluation of data such as the overall fertility rate of women under the age of 25, the average education level of women aged 15 and above, and the per capita income [21]. According to the SDI values, countries or regions were divided into five quantiles: high SDI, medium (high-medium, medium, low-medium) SDI and low SDI. The SDI ranges from 0 to 1 and represents the degree of development related to health outcomes at each study site, with higher numbers indicating higher levels of development.
DALY refers to all the healthy years lost from disease onset to death, including years of life lost due to premature death and years of life lost due to Disability [18]. DALY is an indicator to measure the burden of disease in a specific population and the effect of interventions. It is used to quantify the healthy life lost due to injury or disease. Analysis of DALY distribution in different regions, different subjects (gender, age) and different diseases can help to identify the major diseases with serious risk, key populations, high-risk populations and high-risk areas, and provide important basis for determining the prevention and research priorities.
Estimated average percentage changes (EAPCs) is used to evaluate the ASR trends of morbidity, mortality, and DALY during a specific period [22]. The EAPC and its 95% confidence interval (CI) were calculated using log-linear regression as follows:
y = α + βx + ε, where x represents the year and β is the regression coefficient. The EAPC was determined to be 100 × [exp(β) − 1], and the 95% CI of the EAPC was derived from the standard error generated by the log-linear regression [23]. We interpreted the direction of the trend according to the results of the 95% CI, and the value of 95% CI greater than 0 was considered as an upward trend, and the value of 95% CI less than 0 was considered as a downward trend. If 95% CI is 0, it indicates that the difference in trend change is not statistically significant [24]. This study aimed to estimate the dynamic trends in the prevalence, incidence and DALYs of LLD from 1990 to 2021.
This study considered measures like incidence, DALY, age-standardized rate (ASR), EAPC, and percentage change when analyzing the worldwide burden of disease attributed to LLD. From 1990 to 2021, we examined country-time trends in LLD burden, expressed as average annual percent change (AAPC), across 204 nations and regions throughout the globe using joinpoint regression models. The 95% uncertainty interval (UI) was defined by the 2.5 and 97.5 percentiles. Using the nested Laplacian approximation ensemble Bayesian age-period-cohort (BAPC) model and the age-period-cohort (APC) model inside the maximum likelihood framework, we additionally forecasted the burden of LLD disease from 2022 to 2040. Calculation pole mapping and data cleaning were done using R software (version 4.2.2). The data was shown using the R program “ggplot2” and the photos were compiled and arranged using Adobe Photoshop 2021.
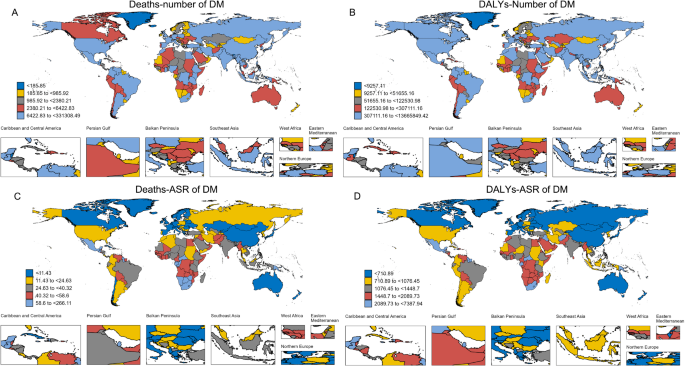
According to reports, the ASIR of LLD is gradually rising globally, rising by 0.01 per 100,000 people annually. However, five SDI regions—High SDI (0, 95%CI -0.08 to 0.08), High-middle SDI (-0.19, 95%CI -0.24 to -0.14), and Middle SDI (0.26, 95%CI 0.2 to 0.33)—showed neither a rise nor a drop in EAPC, based on SDI subregions. Low SDI (-0.22, 95%CI -0.32 to -0.13) and Low-middle SDI (-0.15, 95%CI -0.26 to -0.04) (Table 1). On the other hand, East Asia’s ASIR significantly increased (0.62, 95%CI 0.49 to 0.74). In 2021, Tokelau and Niue had the lowest incidence of LLD (8.45, 95%UI 5.41 to 12.50), while China reported the highest incidence (151.2, 95%UI 119.5 to 190.5) (Supplementary Table S1). ASIR and SDI have a substantial negative connection (p < 0.001), as seen in Fig. 1A. According to ASIR calculations, Brunei Darussalam had the lowest ASIR (0.023, 95%CI 0.016 to 0.034) and Uganda had the greatest ASIR (2.01, 95%CI 1.41 to 2.81) at the national level in 2021 (Fig. 2A). Age-standardized rates for DALYs increased significantly worldwide, rising from 9.243 million in 1990 to 9.805 million in 2021, or 0.03/100,000 year (Supplementary Tables S1, S2). High SDI countries had an EAPC of -0.01 (95%CI -0.08 to 0.07), moderate-to-high SDI countries had an EAPC of -0.11 (95%CI 0.11 to 0.25), middle SDI countries had an EAPC of 0.18 (95%CI 0.11 to 0.25), low-medium SDI countries had an EAPC of -0.1 (95%CI -0.2 to -0.01), and low SDI countries had an EAPC of -0.17 (95%CI -0.25 to -0.08) (Table S2, Supplementary). Spain (1.12, 95%CI 0.86 to 1.38) and the Republic of Korea (1.05, 95%CI 0.68 to 1.42) had the highest growth rates at the national level. On the other hand, Singapore (-1.49, 95%CI -1.68 to -1.3) and Denmark (-0.83, 95%CI -1 to -0.66) had the biggest decreases in DALY rates for LLD (Fig. 2B).

The association between socio-demographic indices and rates. (A) Association between SDI and age-standardized LLD incidence; (B) Association between SDI and DALYs. SDI, Socio-demographic Index;DALYs, Disability-adjusted life years; LLD, Late-life depression

Global burden of disease of LLD in 204 countries and territories. (A) Incidence from LLD; (B) DALYs of LLD. LLD, Late-life depression; DALYs, Disability-adjusted life-years
Of note, Fig. 1B shows that there was a significant linear correlation between ASDR and SDI, but there was no significant trend toward a negative correlation (p < 0.001).
In addition, the Joinpoint regression method combined with APC and AAPC analysis was used to evaluate the trend change of the incidence of LLD in the global and five SDI regions from 1990 to 2021. Globally, the incidence of LLD showed an overall upward trend (AAPC: 0.22), with an upward trend in high SDI (AAPC:0.1), middle SDI (AAPC: 0.45), and low-middle SDI (AAPC:0.18) regions. However, the high-middle SDI area showed a downward trend (AAPC: -0.03), and the trend in the low SDI area showed no significant increase or decrease (AAPC:0) (Fig. 3).

The average annual percent change (AAPC) of incidence from LLD in Global and 5 SDI. SDI, Sociodemographic Index; AAPC, the average annual percent change
The global incidence of LLD rose with age among people over 60 between 1992 and 2021 (Fig. 4A, Supplementary Table S4), with a net drift of -0.02 (95% CI: -0.11 to 0.05) and a significant decline among women (net drift of -0.03; 95% CI: -0.10 to 0.03). Nonetheless, LLD, one of the DALY indicators, decreased gradually with age in both sexes (Fig. 5A, Supplementary Table S3), with women experiencing a larger fall (net drift of -0.01; 95% CI -0.08 to 0.04).

Local drift, age effect, period effect, and cohort effect of LLD’s incidence in Global and in each SDI region from 1990 to 2021. (A) Age effects; (B) Period effects; (C) Birth effects; (D) Age Annual change effects. LLD, Late-life depression; SDI, Socio-demographic Index

Local drift, age effect, period effect, and cohort effect of LLD’s DALY in Global and in each SDI region from 1990 to 2021. (A) Age effects; (B) Period effects; (C) Birth effects; (D) Age Average change effects. LLD, Late-life depression; SDI, Socio-demographic Index
Period effects show that the trends in incidence and DALY rates from 1992 to 2021 are unclear worldwide, irrespective of sex (Fig. 4). In comparison to 1992–1996, the incidence rate and DALY rate peaked in 2002–2006, decreased in 2007–2011, and then decreased in 2012–2016 (Supplementary Tables S3 and S4).
Cohort rates and DALY rates generally decreased for subsequent 10-year birth cohorts from 1892 to 1999 to 1952–1961 and increased following the 1917–1926 cohort (Fig. 4; Supplementary Tables S3 and S4). Compared to the centralized birth cohort (1936–1961), the cohort born in 1936 had a greater risk of incidence and DALY rate. From 1892 to 1936, women had a lower risk of both conditions than men in the cohort prior to the reference group (Fig. 4C). But in the latest group, the risk was higher than for men (Fig. 4C).
The group aged 75–79 had the highest overall values of DALY rate and LLD incidence in terms of annual rate change. Notably, women saw a larger yearly rate of change in the DALY and LLD rates than men did beyond the age of 79 (Figs. 4D and 5D).
While DALY rates for LLD declined with age generally in all SDI subregions (Fig. 5A), the incidence of LLD rose with age in high, high-middle, and middle SDI regions between 1992 and 2021, while low-middle and low SDI regions saw an overall downward trend (Fig. 4A). Remarkably, the extent of change was comparable for men and women and larger for women across SDI regions (Figs. 4A and 5A; Supplementary Tables S4 and S5). Furthermore, the high-middle SDI region (Fig. 4A) showed the strongest trend in incidence with age, while the low-middle SDI zone (Fig. 5A) showed the strongest reduction in DALY rate.
While there was an overall increased trend in the medium and low-medium SDI areas, the incidence rates of LLD and DALY declined in the high, high-middle, and low SDI areas between 1992 and 2021. Notably, in locations with high SDI, women had greater rates of LLD and DALY than males (Figs. 4B and 5B), but in other regions, the opposite was true. On the other hand, the least amount of change was observed in the high-middle SDI zone (Figs. 4B and 5B).
The change in incidence and DALY rates in the 1933–1936 birth cohort that followed the reference group declined significantly in the other SDI regions and increased marginally in the middle SDI region (Figs. 4C and 5C).
The incidence rate and DALY rate in middle and high-middle SDI areas did not vary significantly in terms of annual rate of change. Significantly lower incidence was seen in regions with high SDI. The remaining regions showed an increased trend (Figs. 4D and 5D).
In 2021, the incidence and DALY rate showed an inverse relationship between LLD and SDI. As the economy improves, the total illness burden of LLD is declining. In the 21 GBD regions that were part of the statistics, the worldwide burden of LLD incidence was marginally lower than anticipated. The load of LLD was comparatively steady when SDI values fell between 0.45 and 0.55. In eastern, central, and western sub-Saharan Africa, the burden of LLD was much higher than anticipated; in the high-income Asia-Pacific region, it was substantially lower than anticipated (Fig. 5A). In 2021, the ASIR of LLD was inversely correlated with SDI overall across 204 countries and SDI regions. Of interest, the burden of LLD was relatively stable in areas with low SDI (SDI < 0.25) (Fig. 5B).
Using data from 1990 to 2021 based on ASIR and age-standardized DALY rate, a frontier analysis was developed to provide additional understanding of the incidence of LLD and possible improvements in the DALY rate (Fig. 6). Boundary lines were used to identify the nations and areas with the lowest incidence and DALY rates by SDI. The gap between the observed and potential realized incidence and disability compensation years in a nation is represented by the effective difference, which is the distance from the maximum ASIR and maximum DALY rate in frontier countries (Supplementary Tables S5, S6).

(A) Frontier analysis based on SDI and LLD’s (DALY rate from 1990 to 2021. The frontier is delineated in solid black color. (B) Frontier analysis based on SDI and age-standardized LLD DALY rate in 2021. The frontier is delineated in solid black color; countries and territories are represented as dots. LLD, Late-life depression; SDI, Socio-demographic Index; DALY, Disability-adjusted life-years
For each nation and region, we computed border differences using the 2021 incidence rate, DALY rate, and SDI (Fig. 6, and Supplementary Tables S6 and S7). In general, when SDI increased, the SDI effective differences for incidence and DALY rates tended to remain constant. The ten major nations or territories with the greatest effective differences from their borders were Greenland, Uganda, Palestine, Lesotho, Tunisia, Angola, Gabon, Equatorial Guinea, Greece, and Congo (effective differences range: 8476.86 ~ 6400.78).
The results of this analysis suggest significant absolute and relative income inequalities in the incidence of LLD and DALYs burden (Fig. 7). A comparison of data from 1990 to 2021 shows a relative reduction in health inequalities. The concentration index of incidence decreased slightly in 2021 (Fig. 7A). The slope index analysis of inequality suggested that the gap in incidence between low and high SDI regions decreased from 6134 in 1990 to 5656 in 2021 (Fig. 7B). DALYs concentrations were calculated to change from − 0,12(95%CI -0.14 to -0.1) in 1990 to − 0.14 (95%CI -0.15 to -0.12) in 2021 (Fig. 7C), and the inequality slope index was − 780 in 1990 and − 714 in 2021 (Fig. 7D). All these results suggest a reduction in the burden of inequality in LLD.

Health inequality regression curves and concentration curves for the incidence (A and B), and DALY (C and D) of LLD. LLD, Late-life depression; SDI, Socio-demographic Index; DALY, Disability-adjusted life-year
In order to offer a thorough and comprehensive assessment of the worldwide burden of disease and trends in the incidence of LLD and disability-adjusted life years (DALYs) among persons aged 60 and older from 1990 to 2021, this study used data from the GBD 2021 project. Several important conclusions were drawn.
With an EAPC in ASIR of 0.01%, we first discovered that ASIR and ASDR of LLD in people 60 years of age and older increased gradually in 204 nations and SDI regions of the world between 1990 and 2021. ASDR’s EAPC was 0.03. The regions with low SDI saw the most decline in SDI, whereas the regions with intermediate SDI had the biggest gain. At the national level, the incidence of LLD is in the same direction as previous findings. Due to the large population base in China and the further aggravation of aging, the prevalence of LLD has always been high. Compared with 20 years ago, the prevalence of depression in the older adults population in China has also increased [25, 26]. As Tokelau and Niue have a population of less than 2000, less developed economies, external support dependence, limited infrastructure and employment opportunities, and no epidemiological data on depression, let alone LLD, have been reported for the whole country. As GBD 2021 data are derived from multiple data sources, we speculate that this may be related to Tokelau and Niue’s low economic development, inadequate health system construction, and lack of adequate data collection capacity, leading to missing or incomplete data. The aging rate of the population in the Republic of Korea leads the world, and the proportion of the older adults population continues to rise, increasing the number of potential patients LLD. The incidence of depression in the older adults in Korea is 26%~42.9%, which is significantly higher than that in other age groups [27]. Spain is one of the most aging countries in Europe [28], and the above data all suggest that the DALY of LLD in these countries is high. It is estimated that the prevalence of depression related syndrome in the older adults population of Singapore is about 9.6% and 4.9% respectively [29]. However, there is no literature report on the EAPC of LLD in Singapore and Denmark. It is undeniable that both countries have relatively developed economies and obvious aging populations [28]. The analysis results of this study can provide certain data support.
Subsequent investigation revealed a substantial negative connection (p < 0.001) between ASIR and SDI. While there was no discernible negative connection trend (p < 0.001), there was a substantial linear correlation between ASDR and SDI. This illustrates how socioeconomic development affects the prevalence of LLD worldwide. The aforementioned findings align with those of earlier research [30, 31]. Disparities in local economic growth, social status, education, chronic illness, social support, gender, and other risk variables may be linked to the trend of LLD occurrence in various nations or regions [32]. Notably, social deprivation and a high burden of infectious diseases are more strongly associated with the frequency of LLD in sub-Saharan Africa [33, 34].
Second, we employed age-period-cohort analysis to offer some evidence in favor of the factors that have influenced the DALY rate and incidence of LLD over the previous thirty years. According to this study, the DALY rate dropped as people aged, while the incidence of LLD grew gradually. Those between the ages of 75 and 79 had the greatest overall LLD incidence and DALY rate values. Among these, women are more likely to have LLD, which is in line with findings from earlier research [35]. In the high and middle SDI areas, the incidence of LLD rose with age in contrast to the low SDI area; nonetheless, the low SDI area revealed significant regional features. DALY rates shown a declining trend across all SDI regions. This could suggest that while LLD treatment in comparatively undeveloped nations is falling behind, LLD treatment and intervention in comparatively developed nations are more ideal. Furthermore, the data on the prevalence of LLD disease in various SDI regions still require improvement because the majority of the current research focuses on non-Caucasian populations and European regions [36, 37].
Regarding cyclical impacts, the DALY rate has stayed constant generally, although the incidence of LLD has fluctuated between drop and growth globally since 1992, indicating a little overall decline (Figs. 4B and 5B). Over the past 20 years, diagnosing LLD has been more challenging globally, and antidepressant medication effectiveness in older people may be low because of a range of physical illness burdens [38]. Due to the more widespread application of appropriate medical resource allocation and the development of relevant preventative initiatives, it is noteworthy that the incidence rate and DALY rate in high SDI and high-middle SDI regions exhibit a significant drop [39]. The cycle decline effect is less evident in places with low SDI, primarily because of a lack of resources and the stigma associated with mental health counseling in less developed economies. This results in a significant treatment gap for LLD, which in turn causes a gap in disease prevention, control, and management of LLD [40].
Regarding cohort effects, the current study’s findings demonstrated that, in the birth cohort from 1892 to 1926, the incidence of LLD and the DALY rate continued to decrease globally throughout the course of succeeding generations. The aforementioned downward tendency might be a result of social changes that have reduced the cohort’s exposure rate to LLD cognitive impairment, brain network malfunction, and vascular disease risk [41, 42]. According to current research, older adults are going through a phase of social role transition because they are unable to handle interpersonal and social issues effectively, and a number of other variables exacerbate their psychological stress [43]. Interpersonal factors significantly contribute to the onset and maintenance of LLD symptoms, according to a study on interpersonal psychological relationships [25]. However, the slower rate of cohort decline seen in low SDI areas as opposed to high SDI areas once more emphasizes how socioeconomic disparities in disease risk management in LLD are currently being handled globally.
Our frontier analysis based on recent trends found that both the incidence of LLD and the SDI effective differences in the DALY rate leveled off as SDI increased. At all levels of the development spectrum, there are multiple countries with rates of LLD and DALY that are far from the frontier (with relatively large effective differences from the frontier), suggesting that opportunities to close gaps have not yet been realized. While there are frontier countries for all SDI levels, it is notable that low SDI countries are leading the way with limited resources; It may serve as a model for improving LLD outcomes in various low-resource Settings. Conversely, the observation that some countries with high SDI, such as the United Kingdom and Ireland, lag in performance suggests that the prosperity and health advances resulting from social development may be disrupted by other confounding factors. Future efforts are needed to identify the drivers of LLD burden prevention and control in high-performing countries and the forces hindering progress in lagging countries.
India and China, the two most populous nations in the world, differ greatly in terms of health condition and the distribution of health resources. In the Indian population sample, the median prevalence of late-life depression was 18.2%. Compared to the global median prevalence of 5.4%, this is much higher [44,45,46]. With more than 54.8 million cases, China is currently the second-largest contributor to the worldwide depression burden [47]. LLD, however, is closely linked to much higher healthcare utilization [48] and financial expenses [49]. These results underscored the need to strengthen the architecture of the health care service system for the aged, raise government funding for health care, and improve accessibility to health care in order to further reduce the socioeconomic gap.
Our study includes a number of noteworthy advantages. First, we use a wealth of high-quality data from the 204 nations and territories that were part of the GBD study on the incidence of LLD and DALY rates over a 32-year period. Second, in order to uncover the long-term patterns of the disease and the shifts in the influencing factors, we employed a thorough statistical technique to investigate the age-period-cohort variations in the incidence of LLD and DALY rate. Third, we calculated the worldwide illness burden of LLD, offering numerical information by nation or area and SDI level, which is crucial for directing LLD prevention.
Despite the strengths of this study, it also has certain limitations. First, it is a macro assessment of the epidemiological trends of LLD globally and in 204 countries/regions over a quarter century. As a result, it may not capture the trend at the micro level, especially in relatively large countries or regions, such as the United States and China, which show certain sub-national differences [50]. Second, we did not report the gender burden of LLD in this study. In addition, some other potential drivers may still exist but are beyond the scope of this study. Of note, as GBD estimates are updated annually, we expect that data collection systems and GBD methods will still continue to evolve to address some limitations (e.g., providing subnational estimates).
In summary, the incidence of LLD and disability-adjusted life years have increased globally. The extent of health inequalities has gradually declined over time. Areas with high SDI had the lowest LLD burden, while areas with low and low-middle SDI had the highest LLD burden. Due to the imbalance of socio-economic development, active interventions and strategic measures are urgently needed to further reduce the burden of LLD in middle and low SDI areas.
No datasets were generated or analysed during the current study.
Thanks to all who contributed to the GBD 2021 study.
This research was supported by the Chinese Medicine Research Program of Zhejiang Province (No.2023ZR054 and No.2023ZL464).
The authors declare no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

Fei, Y., Yu, H., Liu, J. et al. Global, regional, and national burden of geriatric depressive disorders in people aged 60 years and older: an analysis of the Global Burden of Disease Study 2021. Ann Gen Psychiatry 24, 22 (2025). https://doi.org/10.1186/s12991-025-00560-2