Dear Nigerians, Because You are Obsessed With Neatness Doesn't Mean You Have OCD
People joke about being “so OCD,” but real OCD is not a personality trait. It is a painful mental health condition that deserves truth. So if you are part of those who claim to have undiagnosed OCD, please read this.
The first thing most people think of when they hear OCD is a clean kitchen. Maybe a person who reorders their bookshelf by height, or someone who washes their hands one too many times. These images are so embedded in popular culture that they have become the whole story, and the whole story is wrong.
Obsessive-Compulsive Disorder is a chronic mental health condition that affects roughly 2 to 3 per cent of the global population, cutting across age, gender, class, and geography.
It is not a fondness for neatness. It is not a preference for routine. It is a neurological loop that traps a person inside their own mind, repeating, doubting, fearing, with no natural exit. Not the kind of loop where you miss your bus and blame Lagos traffic. The kind where your own brain becomes the traffic.per cent
What makes OCD so misunderstood is not just public ignorance. It is the way the disorder has been absorbed into casual language. "I'm so OCD about my desk," someone says, laughing.
The person across the table who actually has OCD says nothing. They've heard it before. They know there's no point. Because explaining mental health in casual conversation can sometimes feel like trying to explain data bundles to your uncle who still thinks Facebook is the entire internet.
What OCD Actually Is
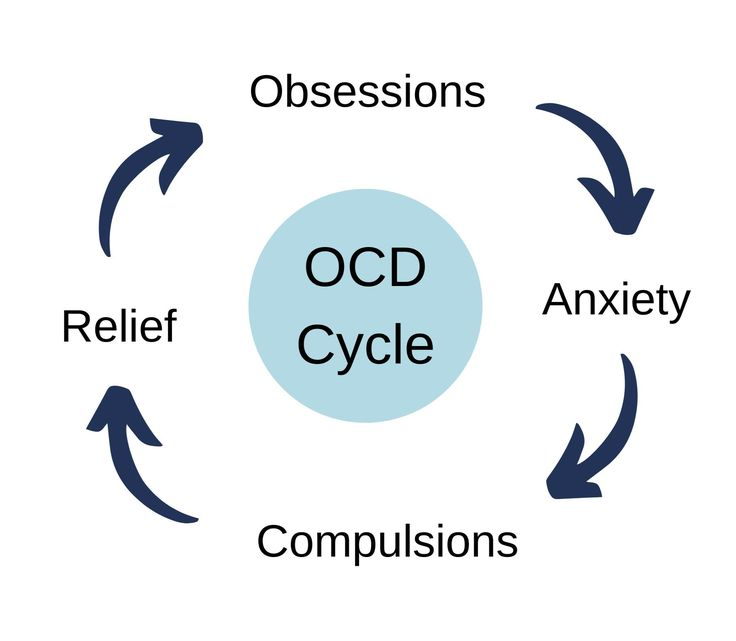
OCD has two components. The first is obsessions, intrusive, unwanted thoughts, images, or urges that enter the mind without invitation and refuse to leave. The second is compulsions, repetitive behaviours or mental rituals performed to reduce the distress the obsession causes. The compulsion does not cure the obsession.
It only quiets it temporarily, which is precisely why OCD becomes a cycle with no end. It is not peace. It is a small generator running during a nationwide blackout, loud, expensive, and not solving the real problem.
The diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), is very precise: the obsessions or compulsions must be time-consuming, taking more than one hour per day, and must cause significant distress or impairment in daily functioning.
A tidy person who likes their desk organised does not meet this threshold. Someone who cannot leave the house for three hours because they must check that the door is locked forty-seven times does. There is a difference between liking order and being imprisoned by doubt. One is preference. The other is wahala with medical documentation.
The Types Nobody Talks About
Contamination OCD
This is the fear of germs and the compulsion to clean, is the only version that gets screen time. But OCD is far more varied, and several of its subtypes are not only invisible, they are actively dangerous because they cause the person suffering from them to believe they are not ill, but evil.
Popular culture looked at one corner of the disorder and said, "Yes, this is the whole mansion." Very impressive work. Very wrong.
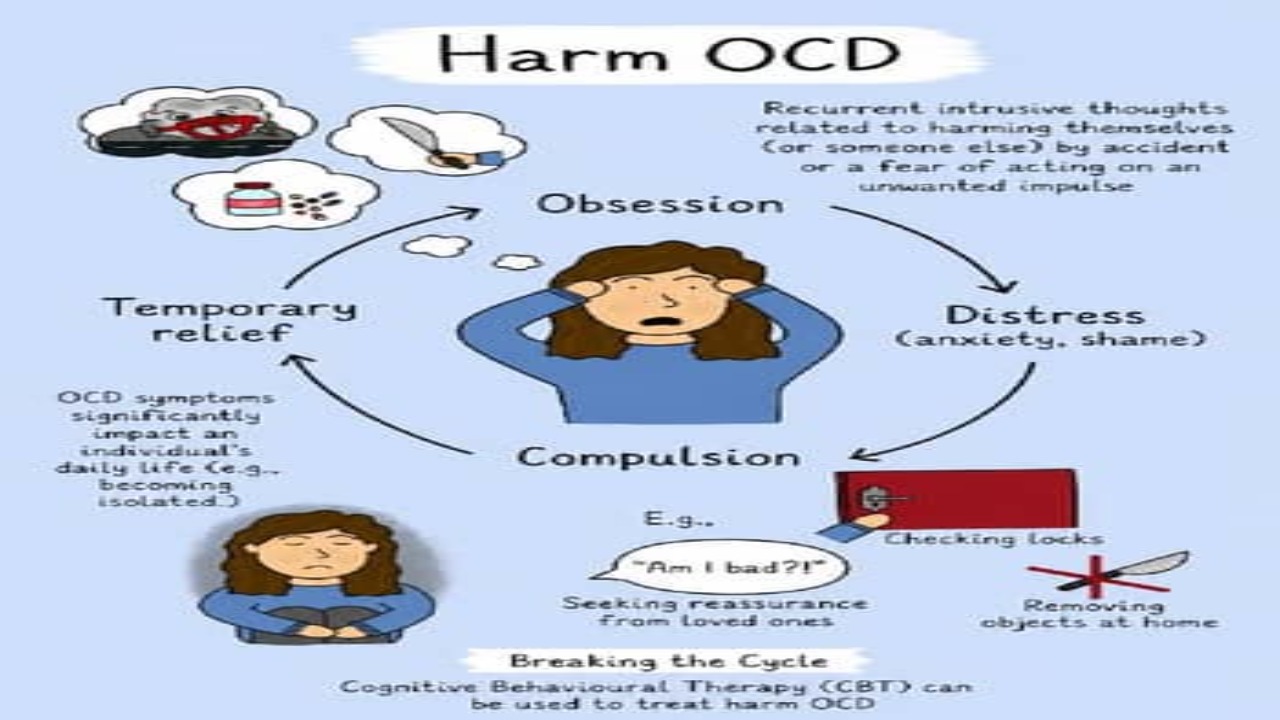
Harm OCD
This involves intrusive thoughts about hurting someone, a child, a partner, a stranger on the street. The person experiencing these thoughts does not want to act on them. In fact, the horror they feel is precisely what defines the condition.
People with harm OCD are statistically less likely to commit violence than the general population, because the thoughts terrify them. But they don't know that. What they feel is shame.
Many never seek treatment because they believe the thoughts reveal something true about who they are. Meanwhile, the actual disorder is sitting in the corner, creating panic like a gossip blog with no fact-checking department.
Scrupulosity OCD
This attaches to religion and morality. The person becomes consumed by fear that they have sinned, blasphemed, or violated a moral code in ways that cannot be forgiven.
They confess repeatedly, to priests, to God, to themselves, but the confession never settles. The certainty they seek never arrives. In deeply religious communities, scrupulosity often goes unrecognised because the behaviour looks like devotion.

In some places, people may even praise it. "This one is very serious with God," they say, while the person is quietly drowning in fear.
Pure Obsessional OCD, often called Pure O, is perhaps the most misunderstood of all, because it produces no visible compulsion.
The rituals are entirely mental: reviewing, analysing, seeking reassurance in one's own head, replaying scenarios to check whether a thought was real or imagined. From the outside, nothing appears wrong.
Internally, the person is running a courtroom trial against themselves on a continuous loop. Judge, jury, prosecutor, witness, and tired court clerk, all inside one head. Even Nigerian election petition tribunals would ask for a break.
Relationship OCD targets intimate partnerships.
The person obsessively doubts whether they love their partner, whether they are attracted enough, whether their relationship is real. They seek constant reassurance, from their partner, from friends, from online forums.
The reassurance helps for minutes. Then the doubt returns. It is not healthy reflection. It is not "checking standards." It is the mind turning love into an interrogation room and then acting surprised when everyone is exhausted.
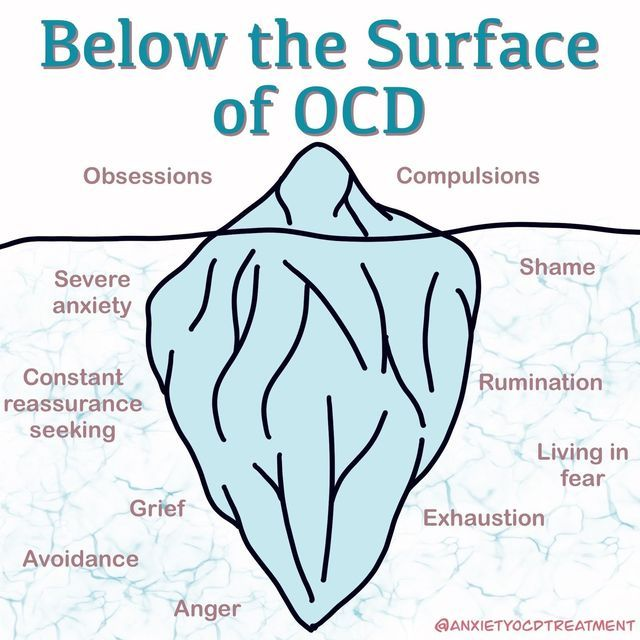
What Does This Cost?
The World Health Organisation (WHO) once ranked OCD among the top ten most disabling illnesses in the world in terms of lost income and diminished quality of life. That ranking came in 1996 and is still cited in clinical literature because the reality it describes has not changed.
People with untreated OCD lose jobs because they cannot meet deadlines while managing rituals. They lose relationships because the reassurance-seeking exhausts the people around them. They lose years. Not minutes. Not small inconvenience. Years. The kind of loss nobody can recover with motivational quotes over a sunset background.
The average delay between the onset of OCD symptoms and the start of appropriate treatment is 14 to 17 years. That number deserves to sit with you for a moment. Nearly two decades of suffering before a person gets help that works, and a significant part of that delay is stigma.
Not just social stigma, but diagnostic stigma: clinicians who dismiss obsessive thoughts as anxiety, or misread compulsions as general stress responses, or who have never been trained to spot the disorder in its less visible forms. Fourteen to 17 years. Some people finish primary school, secondary school, university, NYSC, and still have change left in that time.
In Nigeria and across much of sub-Saharan Africa, the delay is likely longer, because mental health infrastructure is thin and OCD is barely discussed in public health education. The person who is checking and re-checking and cannot stop is told they are anxious, or nervous, or spiritually troubled.
They go to their pastor or imam. They go to their family. They do not go to a therapist trained in ERP, because in many Nigerian cities, finding one is not straightforward. Finding one can feel like looking for fuel during scarcity: everyone has advice, nobody has supply.
The Damage of 'Just Relax'
There is an instruction that people with OCD receive constantly, from people who mean well: just relax. Stop overthinking. Let it go. This instruction is not just unhelpful. In the context of OCD, it is harmful.
Telling someone with OCD to simply not perform a compulsion without clinical support is like telling a person with a broken leg to walk it off. The mechanics of the disorder make voluntary cessation nearly impossible without trained intervention. "Just relax" is not treatment. It is noise wearing perfume.
Worse is when the compulsion-enabling response replaces support. A family member who checks the locks alongside the person to ease their distress, or a partner who offers the same reassurance twenty times because the person keeps asking, these responses feel loving. Clinically, they are called accommodation, and research consistently shows that accommodation maintains and worsens OCD over time.
The person never learns that they can tolerate the anxiety without the ritual, because the ritual always arrives before they find out. It is kindness in the short term, but long-term, it is like giving someone more pepper soup when what they need is actual medicine.
Understanding OCD does not require a medical degree. It requires a willingness to stop flattening a complex disorder into a personality quirk, to stop using it as an adjective for tidiness, and to extend the same gravity to mental illness that we extend to physical disease.
The person who cannot stop the loop in their head is not neurotic. They are not weak. They are ill, and they deserve accurate language around what that means. Accuracy is free. People should try it more often.
What Needs to Change
OCD is treatable. That point matters and should be said plainly. With the right therapeutic approach, primarily ERP, sometimes alongside medication, many people with OCD experience significant relief. Not a cure, because OCD tends to be a chronic condition, but a reduction in symptoms serious enough to allow a functional, meaningful life.
The goal of treatment is not the elimination of intrusive thoughts, which is impossible. The goal is changing the person's relationship to those thoughts, learning to let them pass without responding. The brain may knock on the door. Treatment teaches you that you do not have to open it every time like a nervous landlord.
What has to change, first, is the conversation. Every time someone uses OCD as shorthand for liking clean surfaces, they push an accurate understanding of the disorder further away. Every time a film uses a hand-washing scene for easy character colour without showing the anguish underneath it, the public's mental model stays shallow.
Every time a clinician in a resource-scarce setting misses the diagnosis because the presentation is harm obsessions rather than contamination rituals, a person waits another five years. And because suffering apparently did not already have enough subscription plans.
OCD does not look like a personality type. It looks like a person who is exhausted, ashamed, and convinced that the thoughts in their head say something irreversible about who they are. It looks like someone who has been fighting, privately, for years.
The least the rest of us can do is understand what we're talking about before we talk about it. Which, honestly, would improve public conversation in general, but let us start here.