5 Reasons Why the Drugs That Used to Work on You Have Stopped Working
Why are antibiotics, malaria drugs, and painkillers becoming less effective? The answer lies in five common habits millions of Nigerians practice every day.

There is a particular kind of Nigerian who keeps a small supply of Amoxicillin at home.
For any little headache or body pain, they pop paracetamol, sudrex or Pawafenac, and sadly, this is a global health threat.
With time, the drugs are stopping working, and here is exactly why.
1. You Stopped Taking the Drug Before It Finished the Job
This is the most common and most consequential reason. When a doctor prescribes ten days of antibiotics, and you stop at day five because you feel better, you have not beaten the infection. You have beaten most of it.
The bacteria that survived your first five days of medication are the ones that had some natural resistance to the drug. The weaker ones died first. The tougher ones are still alive.
When you stop early, those survivors wake back up and multiply, having learned something about the drug that killed their neighbours. The next time you take that drug, you are fighting a smarter version of what you were fighting before.
Antimicrobial resistance is fundamentally an evolutionary phenomenon, as pathogens naturally acquire resistance over time.
Every incomplete course accelerates that evolution inside your own body, making future treatment harder for you personally before it becomes a problem for the wider population.
2. Some Bacteria Are Built to Survive Drugs and Wait You Out
Even when you take the full course correctly, there is a subset of bacteria that can survive regardless. Scientists call them persister cells.
Persisters are subsets of a bacterial population that can withstand antibiotic treatment in otherwise antibiotic-sensitive cultures. They typically exhibit slow growth or growth suspension and can restart their growth after the subsidence of a severe stressor.
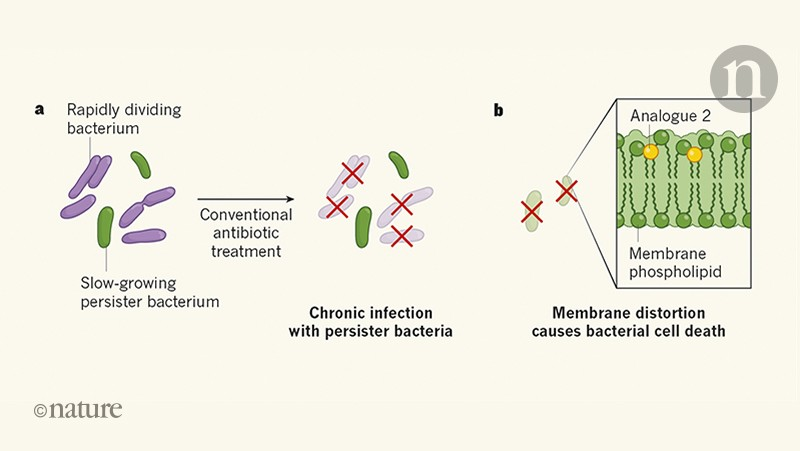
The existence of persister cells can lead to the resilience and resurgence of persistent bacterial infections and the development of antibiotic resistance during treatment.
Think of them as bacteria that go dormant during treatment, like they are simply waiting for the drug to leave the system, and then resume normal activity once it does.
They are not responding to the antibiotic because they have effectively pressed pause. When they restart, they carry whatever resistance mechanisms allowed them to survive, and they pass those mechanisms on.
3. You Have Been Using Antibiotics for the Wrong Thing
Most Nigerians cannot tell the difference between a bacterial infection and a viral one without a lab test. Both produce fev er, body ache, fatigue, and general misery. The common cold, the flu, COVID-19, and most sore throats are viral. Antibiotics do absolutely nothing against viruses.
The AMR challenge is particularly dire in Nigeria owing to the extensive antibiotic use across various sectors and ineffective antimicrobial stewardship programs.
When you take antibiotics for a viral infection, you are not treating the virus. You are exposing all the bacteria naturally living in your body to a drug that selects for resistance among them, without any therapeutic benefit to what is actually making you sick.
The bacteria in your gut, your respiratory tract, and your skin that were not causing any problem are now being exposed to a drug that will kill the susceptible ones and leave the resistant ones behind. You have created resistance in your own microbiome for no reason.
4. Your Body's Nervous System Has Adjusted Its Own Baseline
This one is not about bacteria at all. It is about how your own biology adapts to repeated chemical input, and it applies specifically to painkillers and other drugs that act on the nervous system.
When you take pain medication regularly, particularly opioid-based drugs, your nervous system responds by downregulating its own receptors. It essentially reduces its sensitivity to the drug to compensate for the repeated stimulation.

The same dose that produced significant pain relief on day one produces noticeably less on day ten, not because the drug has changed but because your body has shifted its baseline to account for the drug's presence.
This is called pharmacological tolerance. It is a normal physiological response. It is also how dependency develops even in people who began with entirely legitimate medical need, because the body's adaptation to the drug creates a situation where you need more of it to achieve the same effect, and less of it makes you feel worse than before you started.
5. The Malaria Parasite Is Doing Exactly What the Bacteria Are Doing
Nigeria has one of the highest malaria burdens in the world, and the self-medication patterns around malaria drugs are creating the same resistance problem that antibiotic misuse is creating for bacterial infections, just with a parasite instead of a bacterium.
Artemisinin-based combination therapies are the frontline treatment for malaria in Nigeria. They work within a specific window of the parasite's lifecycle. When people take incorrect doses, stop treatment early because the fever broke, or buy substandard formulations from informal vendors, they expose the malaria parasite to less than a full therapeutic dose.
The parasites caught in the treatment window die. The ones outside it survive, having been exposed to just enough of the drug to begin selecting for resistance without being fully eliminated.

Globally, drug resistance causes an estimated 700,000 deaths each year. If current trends continue, it is projected that by 2050, antimicrobial resistance could result in over 10 million deaths per year and over 100 trillion US dollars in lost output globally.
Malaria drug resistance is a documented and growing component of that figure, concentrated heavily in sub-Saharan Africa.
What You Can Do Right Now
Finish every antibiotic course you start, even when you feel better on day three. Do not take antibiotics for colds, flu, or sore throats unless a medical professional has confirmed bacterial infection. Do not share drugs. When you can access a doctor before medicating, do it.
And treat the malaria drug course the same way you would treat any other: complete, not partial.
The drugs that used to work on you are stopping working because of decisions made daily, by millions of people, inside a system that made those decisions feel reasonable. The system needs to change. So do the decisions. Only one of those things is immediately in your hands.