BMC Psychiatry volume 25, Article number: 492 (2025) Cite this article
Middle-aged and elderly patients with cardiovascular disease (CVD) who have recovered from SARS-CoV-2 infection may experience depressive symptoms due to the physical and psychological impact of the pandemic.
To investigate the prevalence and predictors of depressive symptoms among the middle-aged and elderly with CVD who have recovered from SARS-CoV-2 infection in Wuhan, China, and to develop a prediction model for depressive symptoms.
A cross-sectional study was conducted among 462 former SARS-CoV-2 middle-aged and elderly patients with CVD in Jianghan District, Wuhan, China from June 10 to July 25, 2021. Depressive symptoms were assessed by the Patient Health Questionnaire-9 (PHQ-9). Potential predictors of depressive symptoms were selected by the least absolute shrinkage and selection operator (LASSO) regression. A prediction model was developed by random forest (RF) and logistic regression models and compared by the area under the receiver operating characteristic curve (AUROC). The discrimination, calibration, and practical utility of the prediction model were evaluated by the receiver operating characteristic (ROC) curve, calibration curve, and decision curve analysis (DCA). Bootstrap sampling was used for internal validation.
The prevalence of depressive symptoms among the participants was 35.93%. The prediction model included age, stethalgia after recovery, insomnia after recovery, post-traumatic stress disorder (PTSD), anxiety, fatigue, and perceived social support as predictors. The AUROC of the logistic regression model was 0.909 (95%CI: 0.879 ~ 0.939), indicating good discrimination. The calibration curve showed good calibration. The DCA showed that the prediction model had a net benefit for a wide range of risk thresholds. The internal validation confirmed the stability of the prediction model.
Depressive symptoms are common among middle-aged and elderly CVD patients who have recovered from SARS-CoV-2 infection in Wuhan, China. A prediction model with satisfactory performance was developed to estimate the risk of depressive symptoms among this population. Interventions targeting long COVID symptoms and social support should be considered to prevent depressive symptoms in CVD patients.
Cardiovascular disease (CVD) is the leading contributor to both mortality and premature death in China [1]. The Report on Cardiovascular Diseases in China 2017 showed that more than 40% of deaths in the Chinese population were attributed to CVD [2]. The middle-aged and elderly population is at high risk for CVD, they may also experience serious mental disorders when suffering from CVD as a result of the complex emotional-cognitive adaptations required to manage cardiovascular illnesses, which could negatively impact their overall health [3,4,5]. According to the American Heart Association (AHA), the prevalence of depressive symptoms in patients with CVD was about twice that of those without any disease, and depressive symptoms have been identified as a risk factor for worse prognosis of CVD [4]. In China, a population-based study showed that the prevalence of depressive symptoms and anxiety in CVD patients were 31.9% and 22.3%, respectively, which was over three times higher than those observed in the general population [3]. A study has also shown that the prevalence of depressive symptoms and anxiety could increase substantially with the number of comorbid CVDs [6], which highlights the importance and urgency of prevention and intervention in the mental health of CVD patients.
In late 2019, a novel coronavirus named SARS-CoV-2 emerged in Wuhan, China, causing an outbreak of a respiratory illness known as COVID- 19, and one population that is particularly vulnerable to SARS-CoV-2 infection is the middle-aged and elderly CVD patients who are more likely to have serious complications or even death after infection [7,8,9]. A prospective cohort study conducted during the early period of the COVID- 19 pandemic in Hubei, China indicated that the elderly COVID- 19-infected population with CVD comorbidities had a fatality rate of 39.62% compared with an overall cohort fatality rate of 16.29% due to COVID- 19 infection, and CVD was associated with worse COVID- 19 prognosis [10]. Several retrospective studies conducted during the COVID- 19 pandemic have also suggested that patients with CVD were at a higher risk of various complications when infected with SARS-CoV-2 compared to those without CVD [11, 12]. Furthermore, apart from the COVID- 19 infections caused by the SARS-CoV-2 pandemic, isolation, treatment interruption, and long COVID symptoms such as chronic cough, shortness of breath, chest tightness, cognitive dysfunction, and extreme fatigue, which have further exacerbated the psychological distress experienced by patients with CVD [13,14,15]. A study investigating the mental health of Asian patients with CVD before and during the COVID- 19 pandemic also revealed a notable 11% increase in the incidence of mental disorders among this population due to isolation policies and limited access to mental health and medical care services [16, 17].
The SARS-CoV-2 strain in Wuhan was characterized by high mortality and severe case rates among those infected, which had a profound impact on the mental health of patients infected with COVID- 19 at the early stage [18]. A cross-sectional study conducted from June 10 to July 25, 2021, indicated that the prevalence of depressive symptoms, anxiety, and post-traumatic stress disorder (PTSD) among patients who have recovered from SARS-CoV-2 infection in Wuhan were 36.2%, 27.1%, and 15.2%, respectively [19]. These data demonstrated the substantial impact of the initial COVID- 19 outbreak on the physical and psychological well-being of Wuhan’s SARS-CoV-2 survivors. Among the mental disorders mentioned above, depressive symptoms deserve the most attention [20]. Numerous studies have revealed the relationships between depressive symptoms and COVID- 19 infection. Specifically, Infection with COVID- 19 may lead to inflammatory reactions, physical discomfort, and the emergence of long COVID symptoms, resulting in a decreased quality of life, which can trigger or worsen depressive symptoms [21,22,23]. A retrospective cohort study also showed that patients who have recovered from SARS-CoV-2 may still face a higher risk of mental disorders during the rehabilitation stage after SARS-CoV-2 infection [24]. Additionally, the presence of depressive symptoms may increase an individual’s physical and psychological vulnerability, resulting in a higher likelihood of SARS-CoV-2 infection, hospitalization, admission to intensive care units (ICU), and mortality [25]. Moreover, patients with depressive symptoms have an increased susceptibility to CVD, since such individuals often engage in behaviors associated with cardiovascular risk factors, such as insufficient sleep, physical inactivity, smoking, and alcohol abuse [26, 27]. Therefore, it is crucial to pay attention to the depressive symptoms of patients with CVD who have recovered from SARS-CoV-2 infection.
Despite the World Health Organization’s (WHO) declaration on May 5, 2023, that COVID- 19 no longer constitutes a global health emergency, the challenges of mental health problems for infected individuals revealed during the initial phase of the SARS-CoV-2 pandemic warrant continued attention and evaluation, which could yield valuable insights for managing future potential infectious disease pandemics [28]. Several studies have identified the predictors of depressive symptoms among patients with SARS-CoV-2 infection history. Some studies showed that higher levels of psychological resilience and perceived social support were negatively associated with depressive symptoms; while anxiety and perceived COVID- 19 stigma were positively associated with depressive symptoms among recovered SARS-CoV-2 patients in Wuhan, China [19, 29]. A systematic review indicated that pre-existing psychiatric disorders, colleagues or family members infected, quarantine experience, and physical illness such as cancer, chronic diseases, and persistent physical pain were risk factors for depressive symptoms caused by the infectious disease pandemic among the general population [30]. Another meta-analysis also revealed that sleep disorders were associated with depressive symptoms in COVID- 19 patients [31]. Some studies also developed depressive symptoms prediction models for the sake of improving clinical practice. For example, a retrospective study developed a machine learning model with moderate predictive performance in predicting depressive symptoms among undergraduate students using electronic health records [32]. A systematic review of prediction models for depression risk showed that older age, poor physical health, and cognitive function were the most common risk predictors of depressive symptoms among the elderly [33]. However, few studies have focused on the depressive symptoms among CVD patients who have recovered from SARS-CoV-2 infection. The predictors of depressive symptoms in this population also remain elusive. Additionally, there exists a gap in the literature regarding the development of prediction models for depressive symptoms among them, which highlights the need for further research in this area. The current study is aimed at investigating the prevalence of depressive symptoms among CVD patients who have recovered from SARS-CoV-2 infection in Wuhan, China, paying attention to the middle-aged and elderly due to their vulnerability to both CVD and SARS-CoV-2, and developing a depressive symptoms prediction model with the potential physical and psychological predictors of depressive symptoms. This study is expected to improve the understanding of the key predictors of depressive symptoms among CVD patients influenced by SARS-CoV-2 infection and provide evidence to support the prevention and control of depressive symptoms in the event of future infectious disease outbreaks.
In this study, we have strictly followed the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) statement to report the results [34]. For the sample size estimation, a single-group design was used to obtain a two-sided 95% confidence interval for a single proportion. The simple asymptotic formula was used to calculate the confidence interval. The sample proportion is assumed to be 0.4. To produce a confidence interval with a width of no more than 0.1, 369 subjects would be needed. Anticipating a 20% dropout rate, 462 subjects should be enrolled to obtain a final sample size of 369 subjects. The sample size was computed using PASS 2023, version 23.0.2.
This cross-sectional study was conducted among former SARS-CoV-2 patients in Jianghan District, Wuhan, China, from June 10 to July 25, 2021. According to the electronic medical records of the Health Bureau of Jianghan District, a total of 3059 SARS-CoV-2 patients were eligible for the study and they were infected with the original SARS-CoV-2 strain and were diagnosed between December 10, 2019, and April 20, 2020. Among them, 1601 SARS-CoV-2 survivors were invited for a questionnaire survey on their physical and mental health status when they were receiving clinical re-examination by convenience sampling, and 1541 completed the survey. All investigators and support staff in this study were trained based on the same protocol and were required to have an educational background in medicine or public health. Digital informed consent was obtained from all participants to ensure their voluntary participation.
Self-administered electronic questionnaires and digital consent forms were sent to patients through REDCap, an online survey platform used for delivering online questionnaires. After reading the informed consent form and clicking the “I agree to participate in this study” button on the first page, participants could continue to fill in the electronic questionnaire. The questionnaire consists of demographic characteristics and long COVID-related physical and psychological symptoms. Ethics approval for the questionnaire survey was obtained from the Ethics Review Committee of the Institute of Pathogen Biology, Chinese Academy of Medical Sciences, Beijing, China (IPB- 2020–22). All work involved in this study was performed in accordance with the Declaration of Helsinki. The participants had to meet the following criteria: 1) be equal to or over 45 years old; 2) have a history of SARS-Cov-2 infection; 3) have cardiovascular disease; 4) be proficient in Chinese; 5) be able to independently cooperate with researchers to complete various scale assessments; 6) have mobile communication equipment such as a mobile phone, and a WeChat account; 7) be able to access the Internet with mobile equipment at any time; 8) have not received interventions for mental disorders within 1 month before enrollment or currently in the study. Those who met any of the following criteria were excluded: 1) had serious cognitive impairment; 2) were difficult to cooperate with the questionnaire study. Finally, 462 participants were included in the final analysis based on the criteria above and no missing data was detected in the dataset.
Outcome
The 9-item Patient Health Questionnaire (PHQ- 9) was used for screening participants’ depressive symptoms in the last 2 weeks. This questionnaire was developed by Kroenke in 2001 and has been validated among various Chinese populations [35,36,37]. The PHQ- 9 evaluates the presence of the following symptoms over the previous 2-week period: (a) depressed mood; (b) anhedonia; (c) sleep problems; (d) feelings of tiredness; (e) changes in appetite or weight; (f) feelings of guilt or worthlessness; (g) difficulty concentrating; (h) feelings of sluggishness or worry; (i) suicidal ideation [38]. The items of the PHQ- 9 are scored on a 4-point Likert scale with a range of 0 to 3. A score of ≥ 5 could indicate depressive symptoms. Cronbach’s alpha of the instrument was 0.901 in this study.
Predictors
Participants were asked about their age, gender, weight, region, educational level, marital status, annual income, alcohol use, smoking status, hospitalization of SARS-CoV-2 infection, the SARS-CoV-2 infection status of family members and friends, living conditions, ICU experience due to SARS-CoV-2 infection, psychological counseling status, drug use during SARS-CoV-2 infection, and whether seeking for medical advice due to personal health during SARS-CoV-2 infection.
Participants were asked about their physical symptoms during SARS-CoV-2 infection and after recovery. Symptoms during SARS-CoV-2 infection included fever, respiratory symptoms, gastrointestinal symptoms, and cardiovascular symptoms. Symptoms after recovery included cough, stethalgia, chest distress, dyspnea, headache, fatigue, dysosmia, dysgeusia, loss of appetite, insomnia, alopecia, giddiness, nausea and vomiting, myalgia, and arthralgia.
Psychological symptoms
The Impact of Events Scale-Revised (IES-R) was used to evaluate the SARS-CoV-2-related PTSD of the participants. IES-R is a 22-item scale aiming at screening posttraumatic stress symptoms in adults or older people in the last 2 weeks. The IES-R evaluates the presence of intrusion, avoidance, and hyperarousal symptoms over the previous 2-week period [39, 40]. The items of this instrument are rated on a 5-point Likert scale from 0–4 [39, 40]. A total score equal to or above 35 can be regarded as positive PTSD symptoms. This instrument has been validated in the Chinese population and has been proven valid and reliable among SARS-CoV-2 patients [41, 42]. In this study, the Cronbach’s alpha of the instrument was 0.963.
The Generalized Anxiety Disorder Questionnaire (GAD-7) was used to measure anxiety in this study. The GAD-7 evaluates the presence of the following symptoms over the previous 2-week period: (a) feeling nervous, anxious, or on edge; (b) not being able to control worrying; (c) worrying much about different things; (d) being difficulty in relaxing; (e) being restless; (f) being easily annoyed; (g) being afraid as if awful things might happen [43]. This scale consists of 7 items that are rated on a 4-point Likert scale from 0–3. The scores of the instrument range from 0 to 21. A score of ≥ 5 could indicate anxiety symptoms. This instrument has been demonstrated to be reliable and valid among the Chinese population [44, 45]. In this study, the Cronbach’s alpha of the instrument was 0.948.
The Short Version of the COVID- 19 Stigma Scale (CSS-S) was used to evaluate the perceived stigma caused by SARS-CoV-2 infection in this study. The CSS-S evaluates the presence of personalized stigma, disclosure concerns, concerns about public attitudes, and negative self-image over the previous 2-week period [46, 47]. CSS-S is a 12-item scale modified from the 12-item HIV stigma scale, which has 4 dimensions (personalized stigma, disclosure concerns, concerns about public attitudes, and negative self-image) [46, 47]. CSS-S was initially developed and used in patients with COVID- 19 illness in Lahore, Pakistan, and we translated the English version of CSS-S through a rigorous translation-back translation process. The Cronbach’s alpha of the instrument was 0.932 in this study. We also conducted confirmatory factor analysis (CFA) to validate this scale in the Chinese SARS-CoV-2 survivors in the current study. The CFA model fit indices showed χ2/df = 10.393, RMSEA = 0.085, CFI = 0.937, TLI = 0.930, and SRMR = 0.096, suggesting a good model fit and structural validity of CSS-S. The standardized factor loadings of the 12 items in CSS-S were all above 0.6 and statistically significant. The values of composite reliability (CR) for the 4 dimensions were all above 0.8. The average variance extracted (AVE) of the 4 dimensions were all above 0.6, suggesting good reliability and convergent validity of the CSS-S. The square root of each dimension’s AVEs were all greater than the absolute value of the correlation between this dimension and the other three dimensions, indicating good discriminant validity of this scale. Therefore, we conclude that CSS-S showed good reliability and validity among Chinese SARS-CoV-2 survivors. Each item on the scale is scored on a Likert scale of 1–4. A total score of ≥ 20 indicates a high level of perceived SARS-CoV-2 stigma [48].
The Perceived Social Support Scale (PSSS) was employed to measure the social support level perceived by participants during the past 2 weeks. The PSSS evaluates the ability to perceive material and emotional support over the previous 2-week period [49]. The scale was developed by Li, et al. in 2017 in the Chinese cultural context and has been used among the Chinese MSM population [49]. It contains two items, each scored on an 11-point Likert scale from 0 to 10 (0 = Strongly Disagree; 10 = Strongly Agree). Higher total scores indicated a higher level of perceived support. The Cronbach’s α of the questionnaire in this study was 0.912.
The Resilience Style Questionnaire (RSQ) was used to evaluate participants’ psychological resilience. The RSQ evaluates the ability to successfully adapt to difficult or challenging life experiences over the previous 2-week period [50, 51]. This questionnaire consists of 16 items that are rated on a 5-point Likert scale from 1 to 5. Higher total or mean scores of the 16 items indicate a greater ability to recover from negative events. This instrument was developed and validated among the Chinese [52, 53]. In this study, the Cronbach’s alpha of the instrument was 0.977.
Peace of mind is marked by a serene sense of happiness and a low-arousal positive affect [54]. The Peace of Mind Scale (PoM) was used to evaluate the participants’ levels of a peaceful mind. The PoM evaluates the presence of the following feelings over the previous 2-week period: (a) mind is free and at ease; (b) being content and comfortable with themselves; (c) peace and stability in life; (d) having peace and harmony in my mind; (e) difficulty in feeling settled; (f) living peacefully and comfortably; (g) anxious and uneasy in mind [55]. This scale is composed of 7 items rated on a 5-point scale ranging from 1 (“not at all”) to 5 (“all of the time”). Higher total scores indicate a more peaceful mind. This instrument was validated in the Chinese population and has proven its effectiveness and reliability [55]. In this study, Cronbach’s alpha of the instrument was 0.870.
The Fatigue Scale- 14 (FS- 14) was used to assess the degree of perceived physical and psychological fatigue in this study [56]. This scale is a 14-item scale aiming at measuring the severity of fatigue during the past two weeks [56]. The items of this instrument are rated on a 2-point scale of 0 and 1. Higher total scores on the 14 items indicate a higher level of fatigue. This instrument has been proven valid and reliable among the general population in China [57]. In this study, the Cronbach’s alpha of the instrument was 0.845.
Frequency and percentage were used to describe categorical variables, and mean ± SD was used to describe continuous variables. The whole dataset with 462 samples based on our eligibility criteria was used as the training set. The least absolute shrinkage and selection operator (LASSO) regression was used to select a subset of predictors from demographic characteristics, Physical symptoms, and psychological symptoms that are most associated with depressive symptoms based on the lambda (λ) value that could achieve minimum binomial deviance. The selected variables were further employed in both the random forest (RF) model and backward stepwise logistic regression in the train set. In the RF model, the prediction ability was evaluated by an out-of-bag (OOB) estimate of error rate and classification errors. The importance of each predictor was determined by mean decrease accuracy and mean decrease gini. The predictors in the stepwise logistic regression model were determined based on the Akaike information criterion (AIC). The prediction abilities of the two models were compared by the area under the receiver operating characteristic curve (AUROC) using DeLong’s test and Hanley&McNeil test. The discrimination of the prediction model was evaluated by the receiver operating characteristic (ROC) curve and AUROC. The calibration of the prediction model was evaluated by the calibration curve [58]. Decision curve analysis (DCA) was used to evaluate the practical utility of the prediction model. The bootstrap method with 100 bootstrap sampling was employed to generate an internal validation set, where AUROC, calibration curve, and DCA were used to assess the internal validity of the prediction model. All the statistical analyses were performed using R 4.3.0.
In this study, the average age of 462 participants was (64.71 ± 8.75) years old; 225 (48.70%) were male; 150 (32.47%) were of normal weight; 426 (92.21%) lived in urban; 355 (76.84%) had an educational level of equal or below middle school; 391 (84.63%) were married; 283 (61.26%) had an annual income of less than 60,000 Yuan. 397 (85.93%) were hospitalized due to SARS-CoV-2 infection; 20 (4.33%) had ICU experience due to SARS-CoV-2 infection. 72 (15.58%) had PTSD symptoms; 117 (25.32%) had anxiety symptoms; 418 (90.48%) perceived SARS-CoV-2 stigma; 166 (35.93%) developed depressive symptoms. The details are displayed in Table 1.
In the LASSO regression, the minimum binomial value was achieved when λ equals 0.017, where 12 predictors were selected: age, alcohol use; cardiovascular symptoms during SARS-CoV-2 infection; stethalgia, insomnia, myalgia, and arthralgia after recovery, PTSD, anxiety, fatigue, peace of mind, and perceived social support. Figure 1 illustrates how the binomial deviance and model coefficients change for λ.

Predictor selection in LASSO regression. a: Plot of the binomial deviance test based on lambda value; b: Model coefficients change for lambda value
The variables selected by LASSO regression were used to develop RF and logistic regression models. In the RF model, the error rate was minimized when the number of trees was set as 261. The OOB estimate of error rate was 14.97%, with classification error rates of 10.91% and 22.81%, respectively. The results of the RF model indicated that anxiety and fatigue were important predictors of depressive symptoms, see Fig. 2.
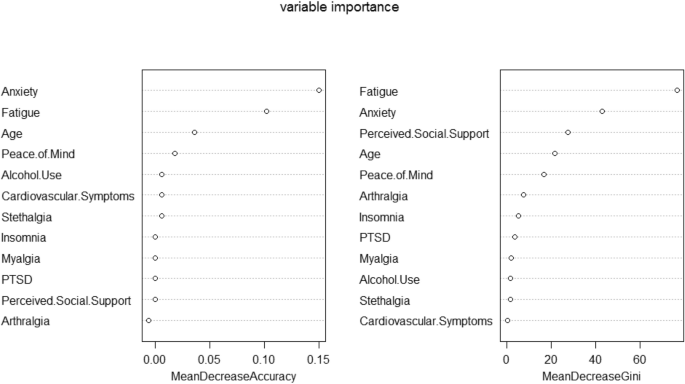
Importance of variables based on random forest model
The results of backward stepwise logistic regression showed that age (β = 0.036, P = 0.029), stethalgia after recovery (β = 0.904, P = 0.093), insomnia after recovery (β = 0.645, P = 0.079), PTSD (β = 1.356, P = 0.006), anxiety (β = 2.926, P < 0.001), and fatigue (β = 0.247, P < 0.001) were positively associated with depressive symptoms. Perceived social support (β = − 0.064, P = 0.010) was negatively associated with depressive symptoms. See Table 2.
The AUROC of the RF and logistic regression models were 0.926 (95% CI: 0.899 ~ 0.952) and 0.909 (95%CI: 0.879 ~ 0.939), respectively. The result of DeLong's test for the two AUROCs was: Z = 1.189, P = 0.234, and the result of the Hanley&McNeil test for the two AUROCs was: Z = 0.896, P = 0.371, both suggesting similar prediction abilities of the two models. Considering the interpretability of the prediction model, the logistic regression model was finally employed in this study to predict depressive symptoms.
The prediction model’s nomogram was constructed using the final predictors determined by the logistic regression model. Points are assigned for each predictor and summed to yield a total score, as indicated by the top of the ruler. The corresponding probability of developing depressive symptoms is displayed below, with higher scores indicating greater risk, see Fig. 3. a. For practical convenience, an online program was created and can be accessed at https://zhenweidai.shinyapps.io/depressionriskcalculator/. After entering the relevant parameters, the risk of developing depressive symptoms can be calculated by clicking the ‘predict’ button, see Fig. 3. b.

Nomogram and online program of the depressive symptoms prediction model. a: Nomogram for predicting depressive symptoms; b: Online program for predicting depressive symptoms
The discrimination of the developed depressive symptoms prediction model was evaluated using ROC curve analysis. The AUROC was 0.909 (95%CI: 0.879 ~ 0.939). The optimal cut-off value of prediction probability was 0.242, with a sensitivity and specificity of 0.880 and 0.797, respectively, indicating good discrimination, see Fig. 4. The result of the calibration curve indicated that the SI prediction model had a good prediction effect requiring no further calibration, see Fig. 5. a. The DCA curve showed that the depressive symptoms prediction model could yield a net benefit to a wide range of approximately between 1.4% and 95.5%, indicating this model is beneficial in making decisions in practical settings, see Fig. 5. b.

Discrimination of the depressive symptoms prediction model. a: ROC curve of the prediction model; b: Cut-off plot of the prediction model

Calibration and decision curve analysis of the depressive symptoms prediction model. a: Calibration of the prediction model; b: Decision curve analysis of the prediction model
Bootstrap sampling was used for the internal validation of our prediction model. The AUROC of the samples in the internal validation set was 0.909 (95%CI: 0.906 ~ 0.912). The optimal cut-off value of prediction probability was 0.275, with a sensitivity and specificity of 0.854 and 0.822, respectively. These values suggest that the discrimination of the model in the validation set is nearly identical to that in the training set. This consistency in performance across different sets further indicated the robustness of our model, see Fig. 6. a. The calibration curve of the internal validation set is shown in Fig. 6. b. The DCA curve of the internal validation set showed that the depressive symptoms prediction model could yield a net benefit when the risk threshold is between 1.3% and 97.9%, See Fig. 6. c.

Internal validation of the prediction model. a: ROC curves of the train and validation sets; b: Calibration of the validation set; c: Decision curve analysis of the validation set
Cardiovascular diseases, such as heart disease and stroke, are more prevalent in older age groups due to various factors, including the natural aging process, unhealthy lifestyles, and the accumulation of risk factors over time [59, 60]. Moreover, research has revealed that patients with CVD are more likely to experience depressive symptoms, and there is an interactive association between depressive symptoms and CVD [61, 62]. Additionally, the elderly and patients with CVD are more susceptible to COVID- 19 infection and experience poorer prognoses, which could exacerbate both physical and psychological well-being [63]. Therefore, we developed a depressive symptoms prediction model with satisfactory discrimination, calibration, practical applicability, and internal validity among the middle-aged and elderly with CVD who have recovered from COVID- 19 infection. The predictors include age, stethalgia after recovery, insomnia after recovery, PTSD, anxiety, fatigue, and perceived social support. Among the predictors, the risk predictors in the model were older age and long COVID symptoms, including stethalgia, insomnia, PTSD, anxiety, and fatigue. The protective predictor in the model was perceived social support. The prediction model could help to estimate the risk of depressive symptoms among this population in practice.
Among the COVID- 19 survivors with CVD history in this study, the prevalence of depressive symptoms was 35.93%, which was higher than that reported among the general population in China during the early stage of the COVID- 19 pandemic [64]. This may be because patients infected with the SARS-CoV-2 experienced negative events such as isolation and discrimination, along with the wide range of symptoms and subsequent treatment caused by COVID- 19, leading to a higher incidence of depressive symptoms [65]. Additionally, the relationship between CVD and depressive symptoms may have a biological basis. A review has shown that inflammation, the abnormity of the hypothalamic–pituitary–adrenal (HPA) axis, and genetic factors may play important roles in mediating this relationship [66]. Furthermore, CVD can impact various aspects of a person’s life, including their daily mood, sense of certainty about the future, and confidence in fulfilling roles. It may also evoke feelings of guilt about past habits that could have contributed to CVD, as well as embarrassment and self-doubt over diminished physical capabilities, which could increase the likelihood of developing depressive symptoms [67]. In addition, individuals with depressive symptoms but no previously detected CVD may have an increased likelihood of developing CVD compared to the general population [68]. This may be due to the presence of uncommonly sticky platelets in people with depressive symptoms, which can accelerate atherosclerosis and increase the likelihood of developing CVD [69, 70]. Evidence has also suggested that in the middle-aged and elderly, depressive symptoms are associated with an increased risk of death and disability [71]. Additionally, cognitive and functional impairment are more prevalent in the elderly with depressive symptoms compared to their younger counterparts [72]. The association between SARS-CoV-2 infection and CVD has also been shown to be considerable. A study has demonstrated a notable association between SARS-CoV-2 infection and CVD, with a long-term increase in the risk of CVD-related complications, such as heart attacks and strokes, even in cases of mild infection [73]. Furthermore, individuals with pre-existing CVD are more susceptible to severe forms of COVID- 19 compared to the general population [74]. Consequently, it is imperative to monitor depressive symptoms in CVD patients to improve their psychological and physical health, as well as the prognosis of both COVID- 19 and CVD.
In this study, the prevalence of PTSD and anxiety among CVD patients were 15.58% and 25.32% respectively, which were all positive predictors of depressive symptoms. A previous study has shown that among elderly patients with CVD, anxiety and depressive symptoms are linked to reduced telomere length, which is a marker of cellular aging that plays a role in the pathogenesis of CVD [75, 76]. In addition, the telomere length is associated with the adverse results of COVID- 19 infection [77, 78]. Senile cells will adopt an inflammatory phenotype and secrete high levels of cytokines, which may lead to more serious symptoms in COVID- 19 rehabilitation patients, which also emphasizes the importance of identifying and predicting depressive symptoms in COVID- 19 rehabilitation patients [77, 78]. Research also indicated that an anxiety reduction could allow individuals to view stressful events as less perilous and intimidating, thereby mitigating negative emotions such as nervousness and decreasing the likelihood of developing depressive symptoms [79]. Considering the psychological impact of anxiety on the middle-aged and elderly with CVD who have recovered from SARS-CoV-2 infection, health authorities could consider implementing interventions for them, such as mindfulness exercises, thought challenging, and graded exposure and systematic desensitization, to improve their psychological well-being and prevent depressive symptoms in this population [80, 81].
During the COVID-19 pandemic, a robust association has been observed between PTSD and depressive symptoms among both CVD patients and the middle-aged and elderly [82,83,84,85]. PTSD symptoms during SARS-CoV-2 infection may be induced by either the immune response to the virus or psychological stress factors. At the initial stage of COVID- 19, the mental health of individuals infected by COVID- 19 was affected due to social isolation, misinformation about COVID- 19, the severity of potential diseases, fear of infecting others, and stigma, which is associated with the occurrence of PTSD after recovery [86]. In addition, the biological association between PTSD and depressive symptoms has been implied by various research. PTSD is associated with dysregulated inflammation, characterized by elevated levels of proinflammatory cytokines such as interleukin (IL)− 1β, IL- 6, and tumor necrosis factor-α (TNF-α) [87, 88]. These dysregulated inflammations could lead to compromised neurocognitive functions, and were also associated with the development of depressive symptoms [89, 90]. Previous research has suggested that PTSD may be also an important risk factor for CVD, given its independent association with adverse cardiovascular health outcomes through biological, behavioral, and societal mechanisms [91]. The interaction between PTSD and depressive symptoms could increase individuals’ distress and dysfunction [92]. Consequently, greater attention should be given to PTSD induced by SARS-CoV-2 among CVD patients. Health authorities could consider implementing professional psychotherapy such as Cognitive Behavioral Therapy (CBT), prolonged exposure therapy (PE Therapy), and stress inoculation therapy (SIT) to help COVID- 19 survivors effectively manage stress and anxiety, and further decrease their PTSD symptoms [93, 94]. In addition, providing active health education to middle-aged and elderly COVID- 19 survivors with CVD is crucial since it can help them understand and accept the adverse events caused by SARS-CoV-2 infection history and CVD, thereby reducing their emotional burden and PTSD symptoms [95, 96]. For patients themselves, encouraging social interaction, regular exercise, adequate sleep, and reducing consumption of harmful substances such as tobacco and alcohol could promote recovery from PTSD [97, 98].
Equally important, insomnia after recovery is another symptom that could contribute to depressive symptoms among CVD patients. The present study revealed a 19.91% prevalence of insomnia among participants, which is higher than the results of meta-analyses conducted on the general population in China both before and during the COVID- 19 pandemic [99, 100]. Studies have shown that the elderly who have recovered from SARS-CoV-2 infection are at an increased risk of developing sleep disorders such as obstructive sleep apnea and insomnia, potentially due to the lack of spousal support, pre-existing mental health conditions, underlying medical issues, negative life events, and acute or recurring psychosocial stressors related to their history of SARS-CoV-2 infection [101]. Moreover, it is particularly imperative to emphasize the negative impact of insomnia among CVD patients, given that insomnia has been shown to confer a 45% increased risk of mortality from CVD in this population [102]. Furthermore, insomnia may exert an influence on the functionality of the brain neurotransmitter serotonin, which has been implicated in the development of depressive symptoms [103, 104]. Insomnia can also affect the body’s stress system, disrupting circadian rhythms and thereby increasing susceptibility to the development of depressive symptoms [105]. Hence, health authorities could consider actively screening for insomnia among the middle-aged and elderly with CVD who have recovered from SARS-CoV-2 infection, and implement interventions aimed at improving their sleep quality to mitigate both the progression of CVD and the development of depressive symptoms [106].
The results of our study suggested that CVD patients with more severe fatigue after recovery from SARS-CoV-2 infection were more likely to develop depressive symptoms. Because of diminished cardiovascular function, fatigue has become one of the most common and distressing symptoms reported by CVD patients [107, 108]. In addition, systemic inflammation, dyspnea, increased metabolic demand, and other kinds of pathogen-mediated damage and physical discomfort caused by SARS-CoV-2 also further led to CVD patients being more prone to fatigue after infection [109, 110]. Studies have shown that fatigue can lead to changes in the systemic immune system and inflammatory changes in the brain, releasing inflammatory mediators such as TNF-α and Type I interferons, leading to excitotoxic damage in the surrounding neuron and an increased risk of depressive symptoms [111]. Moreover, previous qualitative studies also found that fatigue can bring negative emotions to CVD patients such as vulnerability and helplessness, as well as feelings of loss related to their physical energy and their increased dependence upon other people, which could further lead to the occurrence of depressive symptoms [112, 113]. Caregivers can alleviate the fatigue of the middle-aged and elderly with CVD who have recovered from SARS-CoV-2 infection by improving their nutritional status and living conditions, and appropriately increasing physical activity and cardiac rehabilitation interventions [114, 115]. Furthermore, previous studies have described that psychological interventions based on mindfulness or CBT have a positive effect on reducing fatigue and depressive symptoms, and similar interventions can be considered in this population in the future [116,117,118].
In this study, participants with stethalgia after recovery from SARS-CoV-2 were more likely to develop depressive symptoms, which is similar to the results of previous research [119]. SARS-CoV-2 infection could have a negative impact on the progression of CVD in the middle-aged and elderly, and the worsening of CVD is often characterized by stethalgia due to insufficient oxygen-rich blood in the heart muscle [120, 121]. As a result, CVD patients may develop depressive symptoms when experiencing stethalgia since they may be concerned about the negative progression of their CVD caused by SARS-CoV-2 infection and the potential impact of long-COVID on their physical health [122,123,124]. Additionally, a prospective cohort study revealed that depressive symptoms were associated with stethalgia through several biomarkers or biological pathways such as the sympathetic nervous system, the HPA axis, C-reactive protein, ILs, and TNF [125]. Consequently, health agencies may consider implementing regular physical examinations for the middle-aged and elderly with CVD, particularly those experiencing stethalgia after SARS-CoV-2 infection, to timely identify the cause of their symptoms and prevent the progression of CVD as well as the occurrence of depressive symptoms [126, 127].
By contrast, we found that perceived better social support was a protective factor against depressive symptoms among our study population. The COVID- 19 prevention and control measures, such as containment and isolation, have destroyed interpersonal communication and social connections. In this case, social support can protect against depressive symptoms during unexpected crises [128, 129]. Consistent with previous studies, perceived social support plays a crucial role in influencing and improving mental health among CVD patients during COVID- 19 [130, 131]. Those who have a higher level of perceived social support would perceive less social isolation and loneliness, and could more easily perceive the support and care from families, friends, or others, which can buffer stressful life events and adverse circumstances, and serve as an important protector of physical and mental health among the middle-aged and elderly patients with CVD recovering from SARS-CoV-2 [132, 133]. Based on this, the government, health authorities, and people around the patients with CVD recovering from SARS-CoV-2 should adopt multi-dimensional approaches to provide emotional and material support for this population, and encourage them to actively participate in social activities to help patients more easily perceive the support of the surrounding environment, to avoid the occurrence of depressive symptoms [134].
This study has several limitations. First, the causal relationships between the predictors and depressive symptoms in the prediction model cannot be proved considering the drawback of a cross-sectional study. Second, this study only recruited participants who had mobile communication devices, which may cause selection bias. Third, the use of convenience sampling may weaken the representativeness of our research sample. Fourth, the study population was all from Jianghan District, Wuhan, China, and were all above or equal to 45 years old, which restricted the generalizability of the prediction model. Fifth, the model may omit some potential predictors, such as the number of comorbid CVDs and cardiovascular risk factors.
However, this is the first large-sample study to explore the predictors of depressive symptoms among the middle-aged and elderly with CVD who have recovered from SARS-CoV-2 infection, which developed both a nomogram and an online program to predict the risk of depressive symptoms among this population. Further screening of depressive symptoms among the middle-aged and elderly with CVD after recovery from infectious disease could be applied based on the developed model in this study. Interventions targeting insomnia, anxiety, PTSD, fatigue, and social support could be incorporated into personalized plans to mitigate their depressive symptoms. More longitudinal research could be conducted to further assess the generalizability of the prediction model in other context or among different populations, thus optimizing the model with more reasonable and robust predictors.
The prevalence of depressive symptoms among the CVD patients who have recovered from SARS-CoV-2 infection in Wuhan, China was 35.93%. A prediction model was developed to practically predict depression risk among this population. The model indicated good discrimination, calibration, internal validity, and practical utility. Tailored intervention on alleviating long COVID symptoms such as stethalgia, insomnia, anxiety, PTSD, and fatigue, and improving perceived social support should be considered to reduce depressive symptoms among the middle-aged and elderly with CVD who have recovered from infectious disease infection.
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
- AHA:
-
American Heart Association
- AIC:
-
Akaike information criterion
- AUROC:
-
Area under the receiver operating characteristic curve
- AVE:
-
Average variance extracted
- CBT:
-
Cognitive Behavioral Therapy
- CFA:
-
Confirmatory factor analysis
- COVID- 19:
-
Coronavirus Disease 2019
- CR:
-
Composite reliability
- CSS-S:
-
COVID-19 Stigma Scale
- CVD:
-
Cardiovascular disease
- DCA:
-
Decision curve analysis
- FS- 14:
-
Fatigue Scale-14
- GAD-7:
-
7-Item Generalized Anxiety Disorder Questionnaire
- HPA:
-
Hypothalamic-pituitary-adrenal
- ICU:
-
Intensive care units
- IES-R:
-
Impact of Events Scale-Revised
- IL:
-
Interleukin
- LASSO:
-
Least absolute shrinkage and selection operator
- OOB:
-
Out-of-bag
- PE Therapy:
-
Prolonged exposure therapy
- PHQ- 9:
-
9-Item Patient Health Questionnaire
- PoM:
-
Peace of Mind Scale
- PSSS:
-
Perceived Social Support Scale
- PTSD:
-
Post-traumatic stress disorder
- RF:
-
Random forest
- ROC:
-
Receiver operating characteristic
- RSQ:
-
Resilience Style Questionnaire
- SARS-CoV-2:
-
Severe Acute Respiratory Syndrome Coronavirus 2
- SIT:
-
Stress inoculation therapy
- TNF-α:
-
Tumor necrosis factor-α
- TRIPOD:
-
Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis
- WHO:
-
World Health Organization
This study was supported by the CAMS Innovation Fund for Medical Sciences (ClFMS)(Grant No.2023-I2M-2-001)for the State Key Laboratory of Respiratory Health and Multimorbidity.
Ethics approval for the questionnaire survey was obtained from the Ethics Review Committee of the Institute of Pathogen Biology, Chinese Academy of Medical Sciences, Beijing, China (IPB- 2020–22). Digital informed consent was obtained from all participants to ensure their voluntary participation. All work involved in this study was performed in accordance with the Declaration of Helsinki.
The authors declare no competing interests.
Not applicable.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

Dai, Z., Liu, X., Jing, S. et al. Development and internal validation of a depressive symptoms prediction model among the patients with cardiovascular disease who have recovered from SARS-CoV-2 infection in Wuhan, China: a cross-sectional study. BMC Psychiatry 25, 492 (2025). https://doi.org/10.1186/s12888-025-06886-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-025-06886-1