BMC Health Services Research volume 25, Article number: 771 (2025) Cite this article
AbstractSection Background
In the current technology landscape, several individuals electronically stores their health information. The personal health system offers significant conveniences to users, hence enhancing patient satisfaction. Assessing the impact of e-health literacy, personal health system, and patient happiness on enhancing patient satisfaction an essential outcome of health services is crucial for system improvement and clarity. This study sought to assess the impact of patients’ e-health literacy levels, evaluated at a training and research hospital, on personal health systems and patient satisfaction.
AbstractSection Methods
The research was carried out in a teaching and research hospital associated with the Ministry of Health in Malatya province from March 15, 2024, until April 25, 2024. The research was executed with data from 275 people. The data collection form consists of 4 sections.
AbstractSection Results
In the present study, 275 people participated, and 57.8% of them were women. 3.69 were the mean score for the personal health system utilization perception, 92.64 was the mean score for the outpatient satisfaction scale, and 3.63 were the mean score for the e-health literacy scale. E-health literacy explained 2% (R2 = 0.02) of outpatient satisfaction and e-health literacy and outpatient satisfaction explained 30% (R2 = 0.30) of the perception of personal health system use.
AbstractSection Conclusion
Outpatient satisfaction influences individuals’ perceptions of their health system, e-health literacy affects outpatient satisfaction, and outpatient satisfaction serves as a mediator between e-health literacy and personal health system perspectives.
The advancement of internet technology has led to the widespread utilization of mobile health services for accessing health-related information and managing health requirements [1]. With the pervasive utilization of smartphones and enhanced internet accessibility, the notions of e-health literacy and health literacy have become integral to our lives.
The World Health Organization characterizes e-health as the secure utilization of communication technology to obtain health information, health education, and related publications at a reasonable cost [2]. In other words, e-health literacy is defined as the ability to search for and find health information necessary for solving a health problem in electronic resources and to interpret and evaluate the information found [3].
In Türkiye, in the light of technological developments, “e-transformation” has been experienced in health and many web-based services have been developed for citizens to easily access health services [4].
In this direction, the Ministry of Health of the Republic of Turkey has implemented many applications within the scope of Electronic Health (e-Health) such as the Central Physician Appointment System (2010), Medicine Tracking System (2012), “e-Nabız” (2015), Telemedicine (2015), and Barrier-Free Health Communication Center (2016) together with the Health Transformation Program [5]. Among these, the “e-Nabız” application was developed and put into practice as a “Personal Health System” (PHS). PHS is an application that allows individuals and healthcare experts to get to health information collected from healthcare institutions by means of internet-enabled devices and mobile gadgets. This system is a personal health record system where people can access and manage all their health histories from a single point, regardless of where their examination, testing, diagnosis and treatment services are performed [6].
This personal health record empowers individuals to actively manage their health. Thanks to this system, especially people with chronic diseases can take a more active role in monitoring their own health [7]. Personal health records are extensively utilized in member nations of the Organization for Economic Co-operation and Development and the European Union, as well as in countries like the United States of America and Australia [8].
The use of e-health technologies is considered an innovative method to overcome the challenges in the health care system [9]. It is reported that thanks to e-health services, more patients can be reached and healthcare institutions can access patients more easily [10]. Again, thanks to e-health services, it facilitated the management of the COVID-19 pandemic and played an important role in overcoming the pandemic with less damage [11]. Another study conducted in the USA reported that well-implemented e-health tools during the COVID-19 treatment process enabled thousands of patients to benefit from reliable healthcare services in a short time [12]. Today, many member countries of the World Health Organization have e-health policies [13].
As in other service sectors, customer satisfaction is an important issue in the healthcare sector [14]. It is necessary to determine to what extent the health institution can meet patient expectations and investigate how satisfied patients are with the service provided. Health institutions’ success and continuity depend on how much they can meet patients’ wishes and expectations [15]. These are studies that allow management and employees to evaluate themselves from an outside perspective through satisfaction measurements, which are also steps in strategic management. The data obtained from satisfaction studies also provide information on the compatibility of strategies with the corporate philosophy, resources and capacity, and sustainable competition [16].
As services begin to rapidly digitalize in today’s technology environment, it is reported that people’s ability to use the personal health system, which contains many personal health data, is related to e-health literacy [17, 18]. Today, with increasing digitalization and artificial intelligence applications, centralized storage of personal health data is becoming common. The personal health system provides important conveniences to users and these conveniences can increase patient satisfaction. One of the important outcomes of healthcare services is patient satisfaction. In order to increase this satisfaction, determining e-health literacy, personal health system usage and its effect on patient satisfaction is considered important in terms of improving the system and making it more understandable. It is considered that conducting studies in which such applications are evaluated by users will provide important information to developers for the development of applications and for users to benefit more effectively from health service provision.
This study sought to assess the impact of patients’ e-health literacy levels, evaluated at a training and research hospital, on personal health systems and patient satisfaction.
Relational scanning model was used in the design of the study. The reason for choosing this model is that it allows for the multi-faceted (direct and indirect) examination of interactions between two or more sets of variables [19].
This study examined the mediating effect of outpatient satisfaction on the relationship between e-health literacy and personal health system usage perception.
The main hypothesis of the study is stated below:
The study was conducted in Malatya Training and Research Hospital affiliated to the Ministry of Health. The hospital is the largest hospital affiliated to the Ministry of Health in the province and has a capacity of 1055 beds. Institutional permission was obtained for the study. The study data were gathered from March 15, 2024, until April 25, 2024.
For the sample calculation, it was determined that the number of patient applications to adult outpatient clinics (excluding emergency and pediatric outpatient clinics) in the first 6 months of 2023 was 335090. For the study, the weekly average number of patients (12888) was calculated first, and then the 6-week average number of patients (77328) was calculated since the study data would be collected over a 6-week period. In the Epi Info program, the universe was 77328, the expected frequency (using the personal health system application) was 17.7% [20], the confidence interval was 95%, and the margin of error was 5%, and the minimum sample size was calculated as 223.
In line with recommendations for Structural Equation Modeling (SEM) [19, 21], a sample size of 275 participants was recruited to ensure robust analysis.
The data were collected with the help of a questionnaire form consisting of 4 sections. The first part of the questionnaire included a 15-question “Socio-Demographic Information” form to determine the demographic characteristics of the participants.
The second part of the survey form included the e-Health Literacy scale. The e-Health Literacy Scale was developed by Norman and Skinner. The scale was developed to determine the ability of individuals to use health-related information technologies and the interaction between e-health programs and individuals. The scale’s Turkish validity and reliability studies were conducted by Coşkun and Bebiş in the adolescent age group, by Tamer Gencer in the 18–45 age group, and by Uskun et al.in the 18–45 age groups. The scale consists of 8 items and was prepared in 5-point Likert type. It is assumed that as the scale average score increases, the e-health literacy level also increases. The Cronbach’s alpha of the e-Health Literacy Scale was found to be 0.88 in the study of Norman and Skinner, 0.78 by Coşkun and Bebiş, and 0.97 by Uskun et al. [22,23,24,25].
In the third section, the personal health system perception scale was used. The scale was developed by Yalman and Öcel with reference to Bodkin and Miaoulis and Goetzinger et al. according to Turkish standards. The scale was prepared in 5-point Likert format. The scale comprises 23 elements. The investigation by Yalman and Öcel produced a Cronbach’s Alpha value of 0.976 [17, 26, 27].
In the fourth part of the survey, the “Outpatient Satisfaction Scale” developed by Kevenk et al. was used. The scale was prepared in 5-point Likert type and consists of 26 items. The Cronbach’s Alpha value of the scale was calculated as 0.943 by Kevenk et al. [28].
The analyses of the study were carried out with SPSS (Statistical Program in Social Sciences) 25 and AMOS 24 programs. The significance level (p) was taken as 0.05 in comparison tests. The conformity of the data to normal distribution was checked with the Kolmogorov Smirnov Test. Cronbach’s α coefficient was utilized for scale reliability.
Structural Equation Modeling (SEM), a mediation analysis method, was preferred to examine the mediation effect between the scales. Before performing multivariate analysis, multiple normal distribution control of the data was performed using the “Observations farthest from the centroid (Mahalonobis Distance) Menu” in the AMOS program. The skewness value of the model was calculated as 5.131 and since this value was less than 8, it was accepted that it provided a multivariate normal distribution [29].
Pearson correlation coefficient was used to compare quantitative variables since normal distribution was ensured. In order to see the partial mediation effect, after the measurement model was established, the mediation model was established, and the status of the relationship between the variables was checked. Goodness of fit values was checked in model evaluation.
Statistics containing demographic information of the participants participating in the study are given in Table 1 below.
The average age of the participants was 33.98 ± 15.43, and the age distribution range was 18–85. It was determined that 57.8% of the participants were female, 49.8% were married, 31.3% were high school graduates, 21.1% were housewives, 49.8% lived in the city center and 31.6% of the household income was 20 thousand TL or less.
Statistics of the scores of the scales used in the study, their sub-dimensions, and the reliability coefficient of the scale are given in Table 2.
Cronbach’s α values of the scales are exceed 0.70, indicating strong reliability [30]. The average score of the e-health literacy scale was 3.63 ± 0.91, the average score of the personal health system usage perception scale was 3.69 ± 0.83, and the average score of the outpatient satisfaction scale was 92.64 ± 22.74.
The results of the correlation analysis of the relationship between the scales are given in Table 3.
A moderate positive statistical relationship was found between e-health literacy and personal health system (r = 0.520), and a low positive statistical relationship was found between outpatient satisfaction and personal health system (r = 0.226). As e-health literacy scores increase, personal health system and outpatient satisfaction scores will also increase.
A low level (r = 0.239) positive statistical relationship was found between personal health system and outpatient satisfaction. As e-health literacy scores increase, outpatient satisfaction scores will also increase.
SEM analysis was applied as a result of observing the relationships between the scales.
To examine the mediating effect of outpatient satisfaction on the relationship between e-health literacy and personal health system usage perception, a measurement model of the relationship between e-health literacy and personal health system usage perception was first established. After the measurement model, a mediation model was established to see the partial mediation effect between e-health literacy and personal health system usage perception. The diagram of the SEM established in the first model is given in Fig. 1 below;
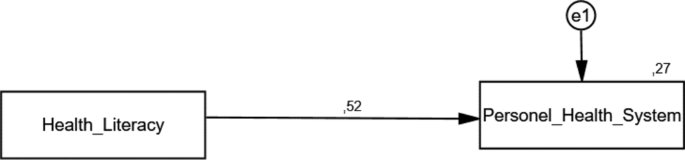
Measurement model of the relationship between e-health literacy and personal health system usage perception
In the model, scale scores are the observed variables and e1 is the error term. In order to interpret the relationships as a result of the analysis, it is first necessary to look at the significance values of the regression coefficients above the arrows drawn between the variables. Table 4 shows the regression coefficients and their significance values.
The effect of e-health literacy on personal health system usage perception was statistically significant (β1 = 0.520; p = 0.001). 27% of personal health system usage perception scores are explained by e-health literacy (R2 = 0.27). If e-health literacy increases by 1 point, the personal health system score will increase by 1.363 (β2 = 1.363; p = 0.001) points. If e-health literacy changes by 1 standard deviation, the personal health system score will increase by 0.520 (β1 = 0.520; p = 0.001) standard deviations. Since the measurement model coefficients were significant, a mediator model was established (Fig. 2).
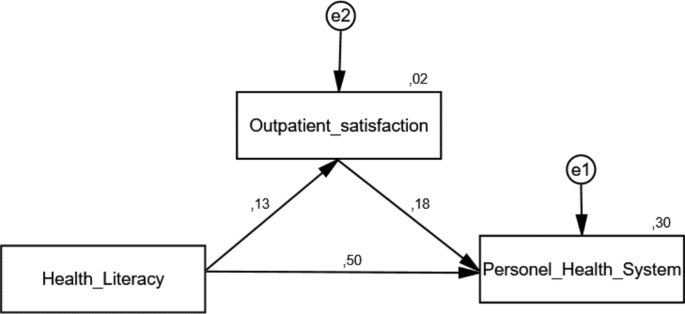
The mediating effect of outpatient satisfaction on the relationship between e-Health literacy and personal health system usage perception
In order to interpret the relationships resulting from the analysis of the newly established model, regression coefficients and significance values are given in Table 5.
The effect of e-health literacy on outpatient satisfaction (β1 = 0.130; p = 0.001) and perception of personal health system usage (β1 = 0.500; p = 0.001) and the impact of outpatient satisfaction on the perception of personal health system usage (β1 = 0.180; p = 0.001) were statistically significant. If e-health literacy increases by 1 point, the personal health system score will increase by 1.304 (β2 = 1.304; p = 0.001) points. If e-health literacy changes by 1 standard deviation, the personal health system score will increase by 0.500 (β1 = 0.500; p = 0.001) standard deviations. If outpatient satisfaction increases by 1 point, the personal health system score will increase by 0.149 (β2 = 0.149; p = 0.001) points. If outpatient satisfaction changes by 1 standard deviation, the personal health system score will increase by 0.180 (β1 = 0.180; p = 0.001) standard deviations. If e-health literacy increases by 1 point, outpatient satisfaction score will increase by 0.393 (β2 = 0.393; p = 0.001) points. If e-health literacy changes by 1 standard deviation, the outpatient satisfaction score will increase by 0.130 (β1 = 0.130; p = 0.001) standard deviations. 2% (R2 = 0.02) of outpatient satisfaction is explained by e-health literacy. 30% (R2 = 0.30) of the perception of personal health system usage is explained by e-health literacy and outpatient satisfaction.
Five thousand samples were reloaded for the bootstrap method to work. If the lower and upper limits of the result obtained in the bootstrap method do not include the zero (0) value, the mediation effect between the variables is statistically significant at the 95% confidence interval [31, 32]. While the effect of e-health literacy personal health system usage perception was 0.52 points in the measurement model, it decreased to 0.50 in the mediation model. The impact of e-health literacy has passed to outpatient satisfaction, with explanatory quality increasing from 27 to 30%. The partial mediation effect between e-health literacy and personal health system usage perception was also found to be statistically significant.
When the results of Bootstrap, a new approach for mediation analysis, were evaluated, it was found that the indirect effect of e-health literacy on the perception of personal health system usage was statistically significant (β = 0.022, GA [0.381–0.602]). It was observed that the Bootstrap lower confidence interval (0.381) and upper confidence interval (0.602) obtained using the percentage method was and it was determined that these values did not include the value zero (0). It was determined that the created mediator model was statistically significant. The indirect effect of e-health literacy on personal health system usage perception through outpatient patient satisfaction was determined to be 0.022.
Whether the established model is verified or not is evaluated in structural equation modeling where multiple fit indices are combined instead of a single fit index with the factors obtained as a result of the research [33]. Upon examination of the fit indices for the defined SEM, the results indicated that the model was statistically significant. The value of χ²/df is 2.356. The quantity of samples utilized to construct the model was deemed sufficient. The RMSEA (Root Mean Square Error of Approximation) was 0.071, with goodness-of-fit indices of 0.98 for GFI, 0.97 for IFI, and 0.98 for CFI (Comparative Fit Index). Given the statistically significant and adequate association between the scales and the established SEM, the multi-group analysis phase commenced [34].
Digitalization has caused significant changes in the delivery of healthcare services. The provision of digital health services has facilitated individuals’ access to health services, increased the effectiveness of health services, and provided significant benefits in improving public health [35].
With the increment in web utilize, electronic health literacy (e-Health) has ended up the focus of attention of healthcare experts [36]. Frequent online searches for health information have been reported to be significantly associated with e-health literacy [37].
Santas et al. found the average score on the e-health literacy scale to be 3.47 (27.82) in their study on university students [38]. Özkan et al. calculated the e-health literacy level as 4.01 in their study among individuals over the age of 18 in Türkiye [39]. Demir et al. found the e-health literacy level to be 3.27 in their study on pregnant women in Samsun province [40]. In their study on personal health system users in Ankara, Uslu and İpek found the e-health literacy level to be 3.76 at a medium level [18]. Kahyaoğlu et al.’s study showed that for healthcare users and healthcare professionals, the e-health literacy level of individuals was 3.54. Özer et al. and Uslu and Şeremet stated that the e-health literacy level was 3.53 and 3.55, respectively [41,42,43]. In their study on bank employees in Tehran, Riahi and Chelak determined that e-health literacy was above average and close to the good point (30.61) [44]. Shi et al. reported that in some studies conducted in China, the perfect e-health literacy score is 40 points and a score of 32 or higher is considered qualified [45]. Özdemir et al. calculated the e-health literacy score as 29.12 in their study on individuals over the age of 15 [46]. In our own study, the e-health literacy level was 3.63 (29.07). The study results are generally similar and indicate that the e-health literacy level is at a moderate level.
The e-health literacy level found as a result of this study is consistent with the study conducted by Shi et al. [45]. The findings suggest that there is still a long way to go to raise it to the level that is considered qualified. Despite increasing technological developments and easier access to information, it has been determined that the e-health literacy level of individuals is not at the desired level. It is thought that it would be beneficial to increase other elements such as digital literacy in order to increase the e-health literacy level of individuals. In this regard, it is thought training and information ought to be provided to extend the e-health literacy levels of individuals.
Uslu and İpek conducted a study on personal health systems users in Ankara province and found that their perception of the use of the personal health systems were at a medium-high level (3.95) [18]. In the study conducted by Yalman and Öcel, participants’ perceptions of using personal health system were 3.72 [17]. In this study, the average score on the personal health system perception scale was 3.69. The difference between the study results is thought to be related to the average age of the individuals in the sample group.
The findings showed that 2% (R2 = 0.02) of outpatient satisfaction is explained by e-health literacy, and 30% (R2 = 0.30) of personal health system usage perception is explained by e-health literacy and outpatient satisfaction. When the Bootstrap results, which is a new approach in mediation analysis, are evaluated, it is seen that the indirect effect of e-health literacy on the perception of personal health system usage is statistically significant and the Bootstrap lower and upper confidence interval does not cover the zero (0) value. The mediator model is statistically significant. It has been observed that e-health literacy has an indirect effect on personal health system usage perception through outpatient patient satisfaction and has a partial mediation effect in this partial effect [31, 47]. With these results, the research hypotheses “H1: E-health literacy has an effect on outpatient satisfaction”, “H2: Outpatient satisfaction has an effect on the perception of personal health system usage” and “H3: Outpatient satisfaction has a mediating effect on the relationship between e-health literacy and personal health system usage perception” were accepted.
Studies suggest that involving patients in healthcare services through patient-centered activities, such as giving simple get to personal health information, improves patient behavior, satisfaction, and healthcare quality and anticipated medical results [48, 49].
Yalman and Öcel examined health literacy and the utilize of e-health services in Düzce province and determined that there was a significant positive relationship between the utilize of personal health system and e-health literacy and stated that the utilize of personal health system could increase the level of e-health literacy [17]. Erkek and Gündoğdu in their study to examine e-health services from the users’ perspective in Konya province, concluded that there’s a weak positive relationship between “knowledge levels” and e-health satisfaction and health service satisfaction [50]. In their study, Uslu and İpek found that the 9% variance in the perception of using the personal health system depends on the e-health literacy level and stated that the increase in the e-health literacy level causes an increase in the perception of use of the personal health system [18]. Alsahafi et al., in their study to determine the components that will influence the acceptance and utilize of the electronic personal health record in Saudi Arabia, expanded the technological acceptance model to incorporate e-health literacy and found that the proposed model clarified 56% of the variance in behavioral intention to utilize the personal health record system [51].
Kim et al. performed a comprehensive review and meta-analysis to ascertain the link between e-health literacy and health-related behaviors, concluding that a favorable relationship exists between the two [52]. In their study, Aydın and Kumru determined that e-health literacy was positively related with the intention to continue using personal health system, an electronic health record system [53]. Rahdar et al. found a positive relationship between e-health literacy level and acceptance of information technologies and sharing personal health records in a study on pregnant women [54]. Since there is a reciprocal relationship between e-health literacy and personal health system usage, increasing the usage of one positively affects the usage of the other. In order to increase e-health literacy and personal health system usage, the level of technological literacy must also be increased.
The study results are limited to patients who applied to a third-level healthcare facility where the study was conducted. It is recommended that future studies include patients admitted to hospitals at different levels and in different regions. Thus, it will be possible to present comparatively the results of patients applying to hospitals of different regions and levels. It would also be useful to measure other parameters such as digital literacy, which are likely to affect e-health literacy.
Research indicates that e-health literacy influences outpatient satisfaction, which in turn affects perceptions of personal health system utilization. Outpatient satisfaction was determined to mediate the association between e-health literacy and perceptions of personal health system usage.
As a result of the study, it was decided that 30% of the personal health system application was explained by e-health literacy and patient satisfaction. According to this result, the importance of increasing e-health literacy and patient satisfaction in disseminating digital health applications, such as personal health system, which is a significant application in reducing the costs of health institutions and providing widespread access to people, emerges. The findings suggest that to increase e-health literacy, public advertisements, scientific studies involving universities, and the Ministry of Health should actively encourage lifelong learning and provide accurate information.
Larger scale studies including diverse demographics and sample sizes on digital systems, including e-health literacy, personal health system, and patient satisfaction an essential health outcome are required. It is thought that these studies will guide the revision of health policies with the changing technological environment with the education and management applied in improving the health of individuals and society.
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
- E-Health:
-
Electronic health
- PHS:
-
Personal health system
- USA:
-
United States of America
- SEM:
-
Structural equation model
- SPSS:
-
Statistical program in social sciences
The summary text consisting of the limited results of this study was previously presented at the "International Malatya Scientific Research Congress" [55].
This research received no external funding.
Ethical approval for this study was received from Malatya Turgut Özal University Non-Interventional Clinical Research Ethics Committee with the letter dated 18.12.2023 and numbered E-30785963-020-192082. The present study was conducted in accordance with the principles of the Declaration of Helsinki.
Informed consent was obtained from all subjects involved in the study.
The authors declare no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The first results of this study were presented as an abstract at the “International Malatya Scientific Research Congress”.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

Koca, M., İnceoğlu, F. & Deniz, S. Determining the relationship between e-health literacy and personal health system and patient satisfaction using structural equation model: an example of a training and research hospital. BMC Health Serv Res 25, 771 (2025). https://doi.org/10.1186/s12913-025-12834-2













