BMC Medical Education volume 25, Article number: 1007 (2025) Cite this article
Ultrasound hip screening is crucial for the early detection of developmental dysplasia (DDH), but little is known about standardized training approaches for nurses. This study aimed to evaluate an educational program combining web-based learning and objective structured clinical examination (OSCE) training to improve nurses’ knowledge and skills in ultrasound hip screening and DDH prevention during universal neonatal and infant home visits.
The program targeted two objectives: (1) to enable nurses to understand the Graf method and acquire standard plane ultrasound images, and (2) to equip them to provide preventive health education on DDH. The intervention included five web-based modules and a two-day OSCE-based hands-on program, supervised by orthopedic pediatric surgeons. Outcomes included (1) knowledge test scores obtained from the web-based modules (range: 0–50 points), (2) OSCE scores (36 items, range: 0–360; global rating ≧3 on a 1–6), including delivery of preventive health education, (3) ability to capture a standard plane image using a phantom within three minutes, and (4) ability to capture a standard plane image with infant volunteers, assessed by medical supervisors.
Nineteen participants (18 public health nurses and one midwife) from three municipalities completed the program. The mean knowledge test score was 47.2 (SD: 2.2), and the mean OSCE score was 329.3 (SD: 21.7), with a global rating of 4.4 (SD: 0.7). All participants conducted the preventive health education component. Eighteen participants (right hip) and 17 (left hip) successfully captured standard plane images using a phantom within three minutes. In scans of 39 infant volunteers, 34 scans (87.2%) successfully captured the standard plane; participants self-reported 31 as successful, though two were objectively classified as failures.
The educational program improved nurses’ ultrasound hip-screening skills and their capacity to deliver preventive health education during universal home visits. These findings support the potential feasibility of expanding nurse-led ultrasound screening and DDH prevention efforts in community settings.
This study was registered with the University Hospital Medical Information Network Clinical Trial Registry before starting the study (No. UMIN000051929, August 16, 2023).
Developmental dysplasia of the hip (DDH) is a spectrum of hip conditions, including malformation of the acetabulum, subluxation, and dislocation. Early detection leads to a low prevalence of acetabular dysplasia in long-term follow-up [1], improves outcomes and quality of life for both children and caregivers, and reduces medical costs [2, 3]. Clinical screening traditionally includes assessments of risk factors such as female sex, breech presentation, and family history [4], combined with physical examination [5]. The Ortolani and Barlow tests are the gold standard in neonatal assessment [6], while leg length discrepancy and limited abduction are useful later in infancy [7]. However, a study has reported that even expert-conducted physical examinations have missed DDH cases [5, 8], and cause late-diagnosed DDH cases [9, 10].
To address these diagnostic limitations, international guidelines strongly recommend ultrasound hip screening for the early detection of DDH [11]. The Graf method is a standardized ultrasound technique for hip screening and provides a noninvasive means of visualizing the immature hip [12]. International screening practices vary considerably [13, 14], with some countries adopting selective screening that prioritizes high-risk cases and other implementing universal screening for all newborns and infants [13]. National guidelines across countries contribute to standardizing screening practices and reducing late diagnoses, particularly in hospital settings [14].
However, the quality of ultrasound screening largely depends on examiner technical skills, underscoring the urgent need for standardized training. Variation in examiner experience and technique can significantly affect image quality [15, 16], and the examiner’s technical skill is crucial for acquiring standard-plane images in the Graf method that can be reliably interpreted by pediatric orthopedic surgeons [17, 18]. Previous studies highlight the importance of improving scanning and diagnostic accuracy through targeted training [19, 20]. Although three-dimensional ultrasound improves image quality compared to two-dimensional devices [21], its adoption remains limited, especially in rural areas where shortages of doctors and healthcare facilities pose major challenges.
To improve access and reduce health disparities, training nurses to perform ultrasound hip screening is essential. Evidence from Mongolia shows that nurses can be trained to perform screening at a level comparable to junior doctors in medical institutions [22]. However, no studies have yet evaluated the implementation of nurse-led ultrasound hip screening during neonatal and infant home visits [23], where diverse home environments introduce additional complexities. Given the critical role of nurses in preventive care and the growing emphasis on task-shifting [24], developing and evaluating standardized educational programs for nurses represents an important area of medical education research. This study evaluated an educational program—including web-based learning and objective structured clinical examination (OSCE)— to train nurses in performing ultrasound hip screening during universal neonatal and infant home visits.
Our preliminary intervention study was conducted in Japan from December 2023 to August 2024. The primary objectives were to (1) train nurses to understand and apply the Graf method of ultrasound imaging for DDH screening and to acquire standard-plane images, and (2) equip nurses to provide health education on DDH prevention to caregivers. Given the public health context in Japan, all eligible nurses were offered the intervention to ensure equitable access to educational resources; randomized allocation was not feasible due to ethical considerations.
The study protocol was approved by the ethics review committee of the primary investigator approved (no. 2023101NI, 28 July 2023; 2023101NI-(1), June 12, 2024), which adhered to the Declaration of Helsinki. Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) guidelines were followed [25]. Informed consent was obtained from all participants via the study website. Both participants and infant volunteers were assigned ID numbers and nicknames to protect their privacy. This study was registered with the University Hospital Medical Information Network Clinical Trial Registry before starting the study (No. UMIN000051929, August 16, 2023) [23].
Participants were recruited through snowball sampling in Okinawa and Aichi prefectures, supported by two pediatric orthopedic surgeons (TK and HT). Of the four contacted municipalities, three agreed to participate. Eligible participants were licensed nurses (PHNs, MWs, or RNs) employed by local governments and actively conducting neonatal and infant home visits. Volunteers without nursing licenses were excluded. Due to feasibility constraints, no formal sample size calculation was conducted. Research funds covered participants’ travel costs.
This program included five e-learning modules (105 minutes) and four two-day hands-on seminars [23]. Based on Gagne’s theoretical framework and the existing ultrasound hands-on seminars of the Japan Society of Orthopedic Ultrasonics, the content covered ultrasound use, hip anatomy, the Graf method, and DDH prevention during newborn and infant home visits [23]. Content was reviewed by pediatric orthopedic surgeons (KA, KF, and TK) and nursing education experts from the Research Institute for Next-Generation Nursing Education (RINGNE).
After completing the e-learning modules, participants attended seminars, practicing probe handling on infant phantoms with normal hip anatomy (Kyoto Kagaku Co., Ltd., Kyoto, Japan) and subsequently on infant volunteers under supervision. Recognizing the limitations of phantoms (e.g., absence of muscle layers, human movements, or crying), orthopedic pediatric surgeons (KA, KF, TK, and TH) recommended hands-on practice with both phantoms and infant volunteers. Volunteers were recruited through snowball sampling, the primary investigator’s laboratory website, and social media. Before practice, pediatric orthopedic surgeons (TK, TH) assessed the safety of infant volunteers. Participant performed two to three supervised scans, followed by two unsupervised scans simulating actual home visit conditions. During unsupervised sessions, surgeons observed but did not provide advice. Following practice, participants underwent an OSCE, and surgeons provided image feedback. Two researchers (any of KYM, HM, CH, MS, MS, and NH) independently evaluated the participants’ skills and provided immediate feedback on areas of improvement [23]. An iViz air Ver.5 linear ultrasound device (Fujifilm, Tokyo, Japan) was used for the screenings in this study.
Knowledge test scores
Participants completed post-module tests assessing knowledge of ultrasound, hip anatomy, standard-plane identification, DDH image classification, and home examination procedures [23]. A passing threshold of (70%–80%) was required to progress. The total score range was 0–50, with data collected from the RINGNE website.
OSCE scores
Participants were evaluated across 36 items covering preparation (8 items), procedure (18 items), standard plane image acquisition (4 items), caregiver education (4 items), and image description and interpretation (2 items) [23]. Each item was scored as 0 (could not be implemented despite advice), 5 (could be implemented with advice), or 10 (could be implemented without advice), for a total range of 0–360 points [23]. Two nursing researchers independently scored the assessments: the average scores was used, and missing values were substituted with one researcher’s score. Completion time for the OSCE and standard plane acquisition was recorded. A six-level global rating scale determined pass/fail status:
Participants at Levels 4–6 were classified as passing; Levels 1–3 as failing [23].
Ability to capture a standard plane image with infant volunteers
Pediatric orthopedic surgeons (TK and TH) assessed the success or failure in acquiring standard-plane images. Success rates for supervised and unsupervised scans and imaging time were recorded. Due to safety considerations, no abnormal hips were included, thus interrater diagnostic reliability was not assessed.
Statistical analysis
Descriptive statistics were calculated for participants’ characteristics, knowledge test scores, OSCE performance, and clinical training outcomes using IBM® SPSS® Statistics for Windows version 29.0 (IBM Corp, Armonk, NY, USA).
Figure 1 shows the flow of participants. Twenty nurses from three municipalities participated in the study; one canceled participation before the e-learning program, and 19 participants successfully completed the entire e-learning and training program. No participants had received training for ultrasound hip screening before.
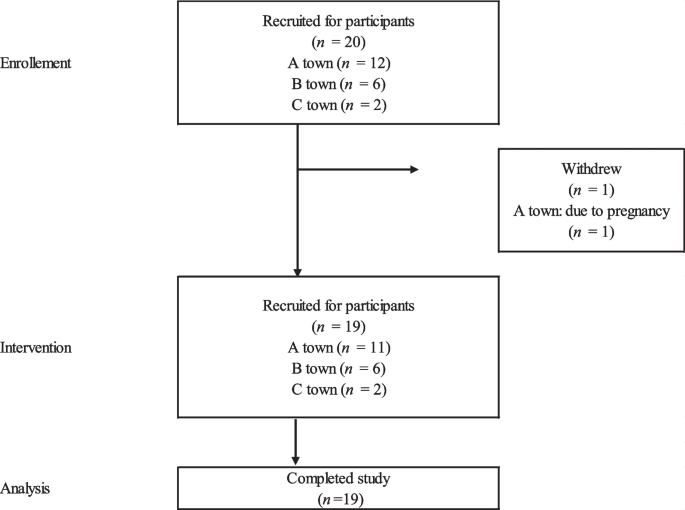
Flow of participants
Table 1 presents participants’ characteristics. Participants’ ages ranged from their 20s to 60s, with the most common age group being 40s (47.4%). Eighteen were engaged in infant home visits as public health nurses and one as a midwife. The average frequency of infant home visits was 1.8 times per month (SD: 1.7, range: 0–7.5).
Table 2 shows participants’ knowledge and skills related to ultrasound hip screening. The mean total knowledge test score on the e-learning was 47.2 (SD: 2.1, range: 43.2–50.0). The mean OSCE score for the checklist item rating was 329.3 (SD: 21.7, range: 272.5–355.0). The mean OSCE score of global rating was 4.4 (SD: 0.7, range: 3–6); One participant was evaluated as level 3 and did not pass OSCE due to failure of imaging the standard plane. All participants completed the OSCE within 20 minutes. The mean global rating was 4.4 (SD: 0.7), with 18 participants (94.7%) scoring 4 or higher and one participant (5.4%) scoring 3. A total of 18 (right side) and 17 (left side) participants self-reported successfully capturing a standard image; 18 (right side) and 18 (left side) participants were confirmed by the researchers to have achieved a standard image. In addition, 18 (right side) and 17 (left side) participants successfully captured standard images within 180 s. The mean time required to capture the standard image among those who succeeded (n = 18) was 86.7 seconds (SD: 67.6) for right side and 71.7 seconds (SD: 62.0) for left side. All the participants completed preventive health education on DDH.
Supervised ultrasound hip screening training was performed 45 times with 9 infants and unsupervised training was conducted 42 times with eight infants. Both hips’ joints were imaged and screened. The mean number of hips examined by participants was 2.5 (SD: 0.8, range: 2–5) with supervision and 2.3 (SD: 1.0, range: 2–6) without supervision. In the unsupervised examination without missing values (n = 39), 34 hips were evaluated to objectively capture the standard plane; 5 of these attempts were unsuccessful. The overall imaging success rate was 87.2%. Participants self-reported that 31 hips were imaging successes. However, two of them were failures when objectively evaluated. (Table 3).
This study evaluated an educational program designed to train PHNs and MWs in performing ultrasound hip screening for newborn and infant home visits. The program directly addressed the need for standardized training, enabling PHNs and MWs—many with limited or no prior ultrasound experience—to acquire essential knowledge and skills. Although ultrasound examinations have traditionally been performed by physicians, particularly in hospitals [10, 12], nurses have recently begun to perform them as well [22]. This study built on that evolving role, demonstrating that trained nurses can perform ultrasound screening effectively even in community-based home settings, which had not been evaluated previously. Expanding this role into home visits has the potential to strengthen early detection and prevention efforts for DDH.
The study found that the mean knowledge test score was 47.2, and 94.7% of the participants passed the OSCE, with a standard plane image acquisition success rate of 87.2%. However, some participants misclassified failed images as successful, highlighting challenges in probe handling and image interpretation, particularly when using the Graf method. Effective probe handling and accurate imaging remain challenging [15, 17]. The Graf method requires precise acquisition of a cross-section through the mid-portion of the bony roof, lower limb of the ilium, and labrum [12]. This underscores the importance of mastering both hip anatomy and probe control, as improper probe angulation can lead to inaccurate images [17, 26]. Although the training incorporated both e-learning and hands-on components, the results suggest that further improvements are needed to close the gap between theoretical knowledge and practical application. Future training should target instruction on recognizing and correcting common imaging errors.
All the participants were able to provide health education regarding DDH to caregivers. DDH is a preventable condition, and caregivers play a critical role in preventing by maintaining the natural flexed position of the infant’s legs through daily practices such as diapering, dressing, baby-wearing, and swaddling [27]. Integrating health education into home visits is an important strategy to enhance preventive impact, and this study supports the feasibility of training nurses to deliver both screening and education [23]. However, further implementation studies are needed to evaluate the effects of such programs on real-world outcomes, including DDH detection rates, caregiver practices, and long-term child health outcomes.
This study has several limitations. First, the sample size was determined by feasibility, and participants were recruited through snowball sampling in selected municipalities, limiting generalizability. Second, the absence of a control group restricts causal inference. Third, while the two-day hands-on seminar format was effective, scaling this format may be challenging to scheduling constraints. Our nurse-specific program was developed to reflect the content of these the Japanese Society of Orthopedic Ultrasonics trainings. Further research is needed to explore whether a shorter, more flexible training can achieve similar effectiveness. Fourth, some participants did not pass the OSCE, indicating the need to investigate barriers to skill acquisition and refine training approaches. Finally, the limited number of orthopedic pediatric surgeons and nursing researchers poses a challenge for scaling the program. Addressing this gap will require developing instructor training and integrating ultrasound screening content into nursing curricula. Additionally, future research could explore ways to further align nurse training with internationally standardized frameworks or certifications to enhance training efficiency and standardization.
This study demonstrated that PHNs and MWs without prior ultrasound experience can successfully acquire essential skills for ultrasound hip screening and preventive health education through a structured training program. Expanding the nursing role into community-based home visits, including ultrasound screening and preventive health education, may strengthen early detection and prevention efforts for DDH cases. Further research is needed to optimize training strategies and evaluate their impact on clinical practice and child health outcomes in community settings.
Research data are not publicly shared because of privacy restrictions.
- DDH:
-
Developmental dysplasia of the hip
- OSCE:
-
Objective structured clinical examination
- RINGNE:
-
Research Institute for Next-Generation Nursing Education
We would like to express our deep gratitude to Emeritus Professor Hiromi Sanada (Department of Gerontological Nursing/Wound Care Management, Graduate School of Medicine, The University of Tokyo; President of Ishikawa Prefectural Nursing University), Professor Gojiro Nakagami (Department of Gerontological Nursing/Wound Care Management, Graduate School of Medicine, The University of Tokyo), Dr. Toshiaki Takahashi (School of Medicine, Yokohama City University), Dr. Yuko Mugita (Department of Next-generation Wound Care Innovation, Graduate School of Medicine, The University of Tokyo), Professor Megumi Haruna (Department of Midwifery and Women's Health, Graduate School of Medicine, The University of Tokyo), Dr. Keiichi Nakagawa (Department of Bioengineering, Department of Precision Engineering, School of Engineering, The University of Tokyo), Dr. Naoki Tomii, Dr. Masayoshi Tsuzuki, and Mr. Ryosuke Oki (Biomedical Precision Engineering Laboratory, Department of Precision Engineering, Faculty of Engineering, The University of Tokyo), Dr. Mari Abe-Doi, Dr. Kazuyuki Komichi, and Ms. Hiroko Yamada (RINGNE) for their valuable contributions and support. We also gratefully acknowledge the Okinawa Association of Child Health and the Aichi Children's Health and Medical Center for their support in facilitating this project.
This research was supported by the Ministry of Education, Culture, Sports, Science and Technology as “Developing a Research Data Ecosystem for the Promotion of Data-Driven Science” (Grant number: none, to Kyoko Yoshioka-Maeda) and JSPS KAKENHI grant as “Development of educational program and implementation for conducting ultrasound hip screening during newborn/infant home visits” (Grant number: 24K02762, to Kyoko Yoshioka-Maeda).
The Research Ethics Committee of the Faculty of Medicine of the University of Tokyo approved the study protocol (no. 2023101NI, July 28, 2023; 2023101NI-(1), June 12, 2024). Informed consent was obtained from all the participants.
We obtained consent for publication from all participants.
The authors declare no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

Yoshioka-Maeda, K., Matsumoto, H., Honda, C. et al. Integrating web-based and objective structured clinical examination training programs for nurses on ultrasound hip screening during neonatal and infant home visits: a case study. BMC Med Educ 25, 1007 (2025). https://doi.org/10.1186/s12909-025-07519-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-025-07519-7