Health Research Policy and Systems volume 23, Article number: 63 (2025) Cite this article
Socioeconomic determinants of health (SDH) account for about 40% of modifiable determinants of health, followed by health behaviours (30%), clinical care (20%) and physical environmental factors (10%). The “10/90 gap” is the idea that only 10% of global health research is devoted to conditions that account for 90% of the global disease burden. For over a decade, SDH research centres have been established in Iran to generate evidence and address SDH.
The purpose of this study was to evaluate the activities and challenges faced by SDH research centres and identify knowledge gaps.
We systematically categorized 759 approved projects (2012–2022) from 29 SDH centres using predefined themes (e.g. mental health, COVID-19, social inequalities). Interrater reliability was ensured through dual independent coding, with discrepancies resolved by consensus. In addition, a bibliometric analysis of 5892 PubMed-indexed articles was conducted using VOSviewer, a validated tool for mapping research trends and collaborations. This phase provided objective insights into publication patterns, keyword clusters and interdisciplinary networks.
Finally, semi-structured surveys were conducted with SDH researchers to identify knowledge gaps and prioritize research areas. Prioritization criteria (e.g. disease burden, equity impact) were scored using a five-point Likert scale, and the results were validated through an expert panel to ensure alignment with real-world challenges.
Out of the 759 approved research projects gathered from 29 reviewed centres, 79 projects were related to mental health, and 53 were related to coronavirus disease 2019 (COVID-19). A total of 5892 articles from 35 research centres obtained by searching PubMed were reviewed and analysed with VOS viewer software. The most frequently used keywords in the centres’ published works are COVID-19, meta-analysis, systematic review, depression, anxiety, and quality of life. In 11 clusters, the 35 research centres under investigation collaborate with 82 additional research centres. Measuring different SDHs at the population level and carrying out related interventions cost far more than the centres’ annual budget. Because of this and other factors stated in the results section, the research centres have shifted their focus to smaller research and more accessible and limited groups and subjects.
There is a mismatch between the subjects that the research centres’ researchers believe should be studied and the approved projects of the centres, as is evident from a review of the centres’ projects and their opinions. Numerous issues may be the root of these discrepancies, such as methods for ranking research subjects, methods for selecting study target groups, how to assess research centres and the different criteria set by colleges and universities.
Social determinants of health (SDH) are non-medical elements that have a major impact on people’s health, wellbeing and quality of life [1]. The circumstances in which people are born, grow, work, live and age, as well as the more extensive range of forces and systems influencing the conditions of everyday existence, are known as the SDH [2, 3]. SDH has a substantial effect on health inequalities, which are the unfair and preventable variations in health status within and between countries. According to a cross-sectional study conducted in countries with different levels of economic growth, the key social factors influencing health were physician density, income inequality, educational attainment and poverty [4]. These factors lead to health inequalities and significant differences in life expectancy among social and economic groups within and between countries [5]. An interesting cross-sectional study conducted in the United States in 2015 revealed that “approximately 40% of modifiable determinants of health are due to social and economic factors, 30% due to health behaviors, 20% due to clinical care, and 10% due to physical environmental factors” [6, 7]. The vital nature of this issue led to the consideration of the term social determinants of health equity (SDHE) and the development of an Operational Framework for Monitoring SDHE [6]. Scholars and decision-makers worldwide should pledge to collaborate on SDH and pool resources from multiple sectors to develop interventions meant to enhance population health [8]. Closing the gap in a generation will be achievable if SDH are addressed systematically and prioritized [3].
SDHE is a primary agenda subject for a variety of national and international documents, including Health in All Policies (HiAP), the Sustainable Development Goals (SDGs) and national and international initiatives to reduce chronic and non-communicable diseases [2].
The emphasis on SDH has steadily increased over the past few decades in national disease programs that cover non-communicable diseases and their risk factors, parliamentary legislation, economic and social development plans and general health policies. Many actions have also been taken in related fields such as standards and environmental health, education, financial aid for vulnerable groups and healthy diet [9,10,11,12]
With a population of more than 85 million people, the majority of whom live in urban areas, Iran is experiencing a rise in the prevalence of non-communicable diseases and risk factors such as diabetes, hypertension, cardiovascular diseases, cancer, mental health issues, substance use and traffic accidents.
To build up the evidence supporting SDH and equity action, a decision taken by the Ministry of Health and Medical Education (MoHME) in 2011 facilitated the establishment of at least one SDH research centre in every province of Iran. These centres have also been developed by several big cities. Each province’s medical science universities gradually established SDH centres. The network of research centres for the SDH secretariat was suggested to be established in 2012. As of 2023, there were 35 research centres extended across 31 provinces in the country, each with 4–18 years of working experience investigating the SDH [13].
The research on SDH across different provinces and the development of appropriate measures can enhance social wellbeing. In recent decades, research has shown that SDH affects population health more than medical care. Therefore, identifying the SDH has become a top priority [13].
Continuous oversight and direction of the evidence-gathering process in SDH priority areas is necessary. The monitoring’s outcomes must identify knowledge gaps and direct studies and interventions to address them.
The WHO plans to develop a unique framework to support researchers in organizing and prioritizing their work. SDH research centres can also use this framework to identify knowledge gaps. The four steps in this guide are plan, implement, publish and evaluate (PIPE). There are several unique substeps in these four stages. Additionally, five categories of studies can be taken into consideration depending on the type of research: studies that quantify the problem, that identify the causes and risk factors, that study solutions and policy options, that study the challenges associated with implementing interventions and policy options and those around monitoring and evaluating the effects of interventions [14].
Given that SDH research centres have been in operation for two decades, we planned to review the research projects conducted in these centres to determine which fields were covered. Have they succeeded in the initial goals for establishing these centres? Finally, identify the knowledge gaps that should be addressed by research centres. In the complementary phase, we investigated the challenges the researchers and centres are faced with while establishing priorities and conducting research in SDH priority areas. The results of the investigation can help countries, particularly developing ones, determine what policies to include in their research agendas to advance priority SDH-related research goals with a minimum of resource waste and challenges.
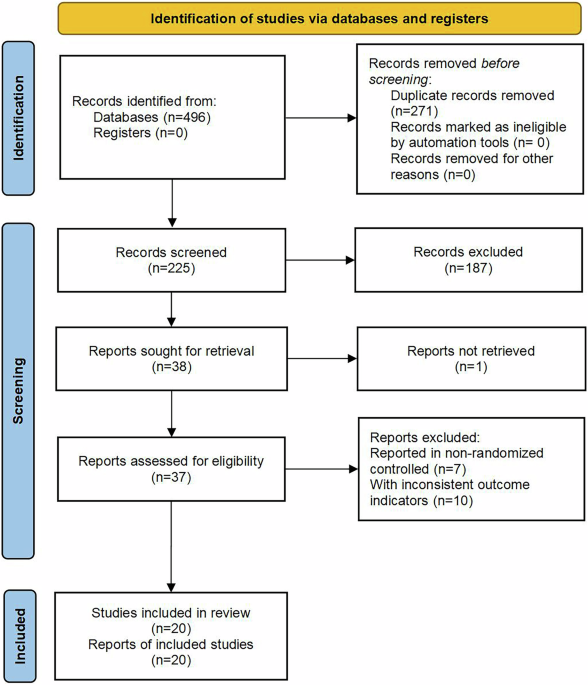
This cross-sectional study employed a multiphase approach to evaluate the research activities of social determinants of health (SDH) research centres in Iran, identify knowledge gaps and determine research priorities. The study was conducted in three complementary phases: (1) collection and analysis of research projects, (2) bibliometric analysis of published studies and (3) identification of knowledge gaps and research priorities through expert consultation (Fig. 1):

Study phases and data used
At first, we communicated with SDH research centres across provinces to introduce and elaborate on the study’s aim to engage their participants in our project. The MoHME is in charge of academic education and health-related research in Iran. To identify SDH research centres, we obtained information on research centres from the MoHME. After that, we communicated with them through phone calls and formal correspondence with the head of each centre. During these correspondences, research proposals were sent to them. We tried to get their support and participation in the project implementation.
A comprehensive dataset of 759 approved research projects from 29 SDH research centres across Iran was obtained. Data were collected through formal communication with the centres, where each centre provided information on its approved projects from 2012 to 2022. The year 2012 was when the law establishing SDH centres was approved. The collected data included:
The research projects were systematically categorized on the basis of thematic areas such as mental health, COVID-19, lifestyle, nutrition, reproductive health and social inequalities. Two independent reviewers manually classified the projects, and discrepancies were resolved through discussion. The frequency distribution of topics, target populations and research approaches was analysed to identify research trends over time.
Bibliometric analysis is a systematic method used to study and evaluate academic publishing [15].
It involves using statistical techniques to analyse patterns, trends and relationships within published literature.
A brief overview of the conducted steps are as follows:
Their publications between 2012 and 2023 in the PubMed database were searched using the affiliation of SDH research centres. The following affiliations were looked up:
Search strategy (((((Social Development & Health Promotion Research Center [Affiliation]) OR (Research Center for Environmental Determinants of Health [Affiliation])) OR (Social Determinants of Health Research Center [Affiliation])) OR (Social Determinants on Oral Health Research Center [Affiliation])) OR (Center for Health Related Social [Affiliation] AND Behavioral Sciences Research [Affiliation])) OR (health equity research center [Affiliation]).
PubMed: 5982 − (1 duplicate + 89 GBD) = 5892.
After extracting 5982 articles and removing 90 articles with multiple authors (global burden of diseases), 5892 articles moved on to the next substeps of the investigation.
Inclusion and exclusion criteria Only English-language articles published between 2012 and 2023 were included; other languages and publication dates were excluded. Articles with multiple authors or GBD-related articles (90 items) that affected the analysis were excluded from the study. The study included all types of articles, including original and review articles.
Data extraction Data were downloaded in comma-separated values (CSV) format. Two authors extracted relevant data independently. The number of documents published during the study period, the centres with the most publications and common clusters amongst centre members were all related.
A qualitative study was designed to identify this phase’s knowledge gaps and research priorities. For doing this, a semi-structured questionnaire (Appendix 1) has been developed to determine the opinion of SDH centre researchers on knowledge gaps in SDH, the challenges of conducting research on the basis of community needs and identifying priorities for research based on the global health research guidelines [1, 2, 5, 13, 14, 16, 17], study objectives and the results of steps A and B. The questionnaire had four semi-structured questions.
Five criteria were used to score question 4: the associated burden of disease, the impact on population health, the potential for implementing interventions, the potential for reducing health inequities and policymakers’ requirement for evidence for evidence-based decision-making. On the basis of the results of the previous steps, potential areas for prioritization were identified, and participants were able to complete this list. Each criterion was scored on a scale of 1 to 5 (1, low; 2, below average; 3, average; 4, above average; and 5, high). The centres graded the criteria for each field, and the priorities were determined using the total criteria’s average score.
At the final step of the study, an Expert Panel with the SDH research centre’s heads was held, and the designed questionnaire was completed at the end of the Expert Panel by the research centres. The Expert Panel were intended to supplement the quantitative portion of the study by gathering comments on the results of Sections A and B. The purpose of the Expert Panel was to better understand the motivations and underlying causes of the current situations and challenges of SDH research. The Expert Panel feedback was sorted into relevant topics after being recorded and transcribed.
To ensure the credibility of the findings:
This study was approved by the Ethics Committee of Tehran University of Medical Sciences. Data were collected with the consent of participating research centres, and confidentiality of unpublished project data was maintained.
Three sections comprise the results: A: analysing all centres’ projects; B: articles and author network analysis; and C: survey results regarding challenges and priorities.
Out of the 759 approved research projects gathered from 29 reviewed centres, 79 projects were related to mental health; 53 to COVID-19; 35 to organizational improvement; 33 to lifestyle; 30 to cancers; 26 to nutrition; 24 to reproductive health and pregnancy; 22 to social support and welfare; 23 to social harm; 19 to addiction; 18 to knowledge, attitude and practices (KAP) in various concerns; and 18 to tool design and their reliability and validity, which made up almost 53 percent of the 759 research projects (Fig. 2). The primary groups researched in various topics are university students, health workers and women (Appendix 1 – Tables 1–5).

Subjects of research that SDH centres focused on
Of the 29 institutions under investigation, centre A (the centres’ names are omitted to maintain anonymity) had the highest percentage of conducted research projects (9.7%) out of a total of 759 projects gathered from 29 research centres. Next, with 66 projects (8.7%), was centre B. Conversely, with eight approved projects, respectively (1% of the total approved projects), centres G and H had the lowest number of projects.
A total of 5892 articles from 35 research centres obtained by searching PubMed were reviewed and analysed with VOS viewer software. The most frequently used keywords in the centres’ published works are COVID-19, meta-analysis, systematic review, depression, anxiety, quality of life, prevalence, mental health and pregnancy and validity. Stated differently, compared with other subjects, the institutes’ researchers have examined COVID-19 and mental health more. Additionally, the words behaviour, obesity, education, self-care, lifestyle and attitude related to the concept of lifestyle. (Fig. 3 and Appendix 1 – Table 6). An overview of the keywords used in association with the study areas can be found in Appendix 1 – Fig. 1–6.

The used keywords of 5892 articles from 35 research centres (left), keywords used in articles around inequality (right)
In 11 clusters, the 35 research centres under investigation collaborate with 82 additional research centres (Fig. 4). The largest and smallest studied clusters were cluster No. 1, which had 21 members, and cluster No. 11, which had three members. Appendix 1 also displays clusters of researchers affiliated with research centres.

Collaborative clustering of research centres
Figure 5 highlights the centres’ major challenges in determining and addressing SDH priorities.

The major challenges the centres had in determining and addressing SDH priorities
The annual funding of research centers, particularly SDH research centers, is insufficient to undertake a province-wide survey. Measuring different SDHs at the population level and carrying out related interventions cost far more than the centers’ annual budget. Because of this and other factors stated below, the centers have shifted their focus to smaller research and more accessible and limited groups.
The annual evaluation of research centres is mostly based on article publication and the H index. This evaluation has an impact on the centres’ annual budget. Therefore, this evaluation method has led centres and researchers to studies that reach the output of the article faster. Due to their availability and concepts that are not SDH priorities, students and health workers have been examined more than vulnerable populations and priority issues.
The mission and aims of the SDH research centres were defined at the time of the centres’ founding by the efforts of the most prominent individuals. However, the centres’ activities were not directed by the annual revised national operational strategy and roadmap in the following years. When directing the SDH research centres, the operational plan and national road map might be valuable tools for the upstream institutions’ evaluation processes.
Since 2015, there has been an improvement in the national and provincial levels of data gathering about diseases and risk factors for diseases; two instances of this improved state of affairs are STEPS and NASBOD. SDH data have been collected in Iran by several ministries, but access to data centres is restricted and there is no conceptual structure and platform to guide this data collection. These conditions have made the determination of research priorities not based on statistics.
Further, centres have invested financial and human resources to measure the status of specific SDH indicators in their provinces; however, the data are not collected coherently and are not easily accessible. The availability of the SDH database can highlight data gaps and aid in addressing the provinces’ data challenges. A lack of accuracy in determining SDH research priorities has resulted from the SDH database’s incoherence.
C-1-e: other challenges faced by research centres in setting priorities for SDH research are being unable to provide a reliable definition of the province’s SDH needs, insufficient understanding of SDH factors from the perspective of top-level managers in both the health and non-health sectors and weakness of ability to knowledge translation.
The lack of clear national and provincial common priorities (23 votes), the absence of a compelling communication network between the centres (22 votes) and the unfavourable procedures or legislation to establish a joint interprovincial study (19 votes) are the main obstacles that the SDH centres face in advancing cooperation and collaborative studies with each other.
SDH factors in the provinces that have had a significant impact on health inequalities are displayed in Fig. 5. In the opinion of SDH centres, the key factors driving health inequalities in the provinces are economic trends, inflation, poverty and inequality of provincial income distribution. Next on the list of causes affecting the health of society and affecting several provinces are drought, climate change and water shortages. According to the experts of SDH centres in the provinces, other factors that greatly impact health inequalities are unemployment and false employment, environmental pollution, air pollution, marginalization, housing and urban development, immigrants, food insecurity and traffic accidents, Fig. 6.

SDH factors in provinces that have a high impact on health inequalities
On the basis of criteria including relevant disease burden, the need for evidence by policymakers to support evidence-based decision-making, the impact on population health, the feasibility of implementing interventions and the potential to reduce health inequalities, SDH centres were graded. Research themes and priority research themes were identified. The priority theme was determined by considering housing and economic policy, as well as inflation, unemployment and wealth distribution. The second priority theme includes food inflation, hunger and food security. Other priority research themes can be seen in Fig. 7.

Prioritized research areas
There is a mismatch between the subjects that the research centres’ researchers believe should be studied and the approved projects of the centres, as is evident from a review of the centres’ projects and their opinions. Numerous issues may be the root of these discrepancies, such as methods for ranking research subjects, methods for selecting study target groups, how to assess research centres and the different criteria set by colleges and universities. The SDH field needs an integrated information and communication network.
There are significant inequalities in health between and within countries and populations, and these disparities are mirrored in the funding and benefits of health research. Since its founding in 1998, the World Health Research Forum has made closing the “10/90 gap” the highest priority. The 90/10 gap has come to represent the mismatch between investments made and research needed, even though it is not yet a measurable metric. The “10/90 gap” is the idea that only 10% of global health research is devoted to conditions that account for 90% of the global disease burden [18].
According to a methodological review conducted between 2001 and 2014, the following approaches were used to set priorities for health research among 165 relevant studies: the CHNRI method was most often used (26%), then the Delphi method (24%), the James Lind Alliance method (8%), the combined approach matrix (CAM) method (2%) and the Essential National Health Research method. (less than 1%). Roughly 3% of the studies reported unclear procedures and scant details regarding the process of determining priorities [17]. Using a combination of criteria for rational priority setting is recommended, including evidence-based medicine, disease burden analysis, cost-effectiveness analysis and equity analysis [16].
One of the World Forum’s main tenets is equity in health research to promote health equity. A tool known as the combined approach matrix (CAM) was created by the World Health Research Association in light of the significance of giving health research top priority to accomplish this goal. The idea behind CAM is to combine many variables in various dimensions into a single analysis tool. The WHO five-stage approach, which connects disease burden to determinants, knowledge of interventions, cost-effectiveness and funding flows, served as the basis for development [19].
An improved version of this tool is now a 3D CAM. After much experience with CAM applications, it became evident that additional dimensions were required to fully capture the variety of discriminatory, marginalizing and vulnerable practices outside of the two core dimensions. This is necessary to guarantee that research is prioritized to maximize benefits to the greatest number of people while promoting equality and better health. Adding an equity component into CAM enhances its awareness of the root causes of the 90/10 disparity. It integrates determining priorities with the rights-based health approach embodied in the SDH research centres and the WHO Charter [19, 20].
Determining neglected areas and allocating funds for research, which leads to improved interventions for the most vulnerable populations, are the goals of prioritizing research. Prioritizing research on the basis of scientific evidence makes it simpler to justify the proper distribution of funds, including a significant movement toward previously underdeveloped areas. Prioritization tools have been created for this reason. These tools’ dimensions and criteria ensure that they account for the social and economic environment, risk factors and disease statistics, power and values structure, and interventions’ cost-effectiveness. Three-dimensional CAM, for instance, considers variables in 3 axes: justice, organizational dimensions and public health; it has 10 subdimensions. With this tool, SDH centres may ensure that the various study groups and issues are properly prioritized [21, 22].
Although the researchers at the research centres were aware of the key components of SDH and its related vulnerable populations, they had dealt with some issues that did not align with the priorities. This is just one part of the story, as we saw in the findings (Fig. 1 and Fig. 5). There are several causes for this diversion from the goals, including the assessment of centres on the basis of their rapid publication of articles rather than taking into account the community’s requirements and initiatives. Respecting these priorities and considering them in the processes of resource allocation and evaluations are the responsibilities of the Vice Chancellor of Research at the MoHME as well as the university, financing and evaluation institutions of research centres [23]. Research priority-setting processes and tools should be designed to (i) classify, arrange and display the copious amounts of data incorporated into the process; (ii) recognize the gaps in health research; as a result, (iii) help determine the priorities for health research on the basis of a procedure that should involve key stakeholders and take the participants’ context and values into consideration [24].
For the first time, CAP was applied nationally and internationally in countries such as Bolivia, Argentina, India and Pakistan, and a set of research priorities for the ensuing years was established [25,26,27,28]. Here are some instances of how the CAM is used to determine research priorities: prioritizing pharmaceutical research for the European Union is a program of the WHO’s European Office [29]. Strategic research strategy prepared by the Malaysian MoHME [30] identifying children’s nutritional priorities in Asia and Latin America [31, 32]. The CAM Health Research Association of Argentina established research priorities in fields such as maternal mortality, traffic safety [31, 32], human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) and tobacco addiction [33,34,35,36].
Biases in the studies’ target group selection had occasionally surfaced, as we saw in the findings section, resulting in the study being done in groups that were most likely not priorities. Frameworks have been established to lessen these biases; one such framework is the BIAS FREE framework. The choice of target groups must be considered while assessing research institutions and projects. It follows that the work of researchers on marginalized, vulnerable and harder-to-reach populations will inevitably result in solutions that improve the health and wellbeing of these populations and lessen the burden of disease on them.
The BIAS FREE Framework, an analytical tool for identifying and eliminating biases in research, was developed, published and released with assistance from the Global Association for Health Research. This framework tackles a variety of discriminatory practices caused by biases against populations on the basis of their gender, sexual orientation, age, class, caste, socioeconomic status, religion or disability. A total of 19 questions comprise the BIAS FREE framework, divided into 3 primary problem categories: upholding hierarchy, neglecting to consider differences and applying differential treatment. Analytical questions challenge users to identify biases in research, policy, programs, service delivery and practice, and suggest solutions to prevent and counter such bias [37, 38]. These experiences should be utilized through SDH centres at both the national and provincial levels.
Three key axes, including governance and leadership, article output (as main key criteria) and impact, have been examined in evaluating the research and technology activities of medical science research centres, and the weight of these axes is the same for all centres. The philosophies of research centres and their areas of work are vastly different. Articles in pharmaceutical research centres are mostly published in high-impact journals, and assessing all centres using the same criterion will cause them to fall short of their initial objectives. The acts and research of SDH centres are such that they manifest themselves over time; as a result, the centres shift toward research in accessible fields with a higher possibility of publication. For example, while social and economic inequalities during COVID-19 faced more challenges to the health of vulnerable groups than before, SDH centre studies focused on non-SDH topics and accessible groups.
Research centres had to overcome three main challenges to promote complementary and collaborative studies. The first issue is that the SDH sector’s national, regional and provincial priorities are unclear; second, the communication network among research centres is weak. The third challenge that research centres face is procedural and legal issues in approving joint research.
Provincial research priorities can be established for each province using a standard methodology by using 3D CAM or comparable tools. The centres in the adjacent provinces might determine shared regional priorities by determining the provincial priorities. Among the challenges mentioned is the network of communication between research centres.
According to an analysis of the clusters of the authors of the centres’ articles, the SDH centres’ researchers have formed 11 clusters or groups of researchers on the basis of their prior acquaintance and cooperation history. Strategies to increase collaboration amongst research centres can be implemented through a variety of channels, including social media, online platforms and regular conferences [39,40,41,42]. It is felt that a research chair is necessary since SDH studies are multidisciplinary. A research chair is a type of collaborative scientific, social network that researchers from different fields integrate. For instance, more than 2400 multidisciplinary researchers collaborate in 125 research chairs established in Mexico. One such chair is in medical engineering, which unites specialists in the fields of mechanical, electrical and medical engineering. Politics, sociology and economics researchers collaborate under a research chair in border studies. Along similar lines, experts from psychology, information technology and education collaborate under a research chair in student learning [42]. With many centres and their activities complementing each other, it makes sense for those involved in the field of SDH research to have a research network that directs the activity of all the centres on the basis of evidence and collaborative decision-making, as well as an active secretariat that plans and monitors the network’s activities.
The present study aimed to guide the research efforts of centres specifically working on social determinants of health (SDH) within the framework of the Ministry of Health and Medical Education (MoHME). Focussing on these centres can have significant positive impacts, as they play a crucial role in influencing health policies and interventions. By aligning their research priorities with the most pressing SDH issues, these centres can effectively contribute to improving public health outcomes.
However, this study had some limitations. It only included researchers and research centres affiliated with the MoHME. SDH is a broad area, and many organizations and research centres across the country might also be engaged in SDH-related studies, which were not covered in this research. This study focussed on the perspectives of SDH researchers within the MoHME regarding research priorities. Although they are highly influential in setting SDH research agendas, insights from other researchers, practitioners and stakeholders could provide a more comprehensive understanding of the priorities. Future studies are recommended to adopt a qualitative approach to explore the viewpoints of other relevant organizations – such as road traffic police, water and agriculture departments and environmental protection agencies – on SDH research priorities.
Research centres, particularly SDH research centres that study wide and multidisciplinary areas, need evidence-based guidance to be effective. Countries should use the existing guidelines, some of which were mentioned in this study, to prioritize research areas and target groups as valuable experiences to help guide their research in each area. The challenges that have prevented SDH research centres from operating at maximum effectiveness have been identified in this study to modify the focus of health research.
On the basis of the study’s findings and the perspectives of SDH researchers, the following strategies are proposed to enhance the way SDH is addressed.
No datasets were generated or analysed during the current study.
- SDH:
-
Social determinants of health
- SDHE:
-
Social determinants of health equity
- SDGs:
-
Sustainable Development Goals
- MoHME:
-
Ministry of Health and Medical Education
- PIPE:
-
Plan, implement, publish and evaluate
- CAM:
-
Combined approach matrix
The research team would like to express gratitude to all the organizations and individuals, whose contribution to advancing SDH and health in all policies in Iran has been remarkable.
No specific research grant was sought or obtained for this study.
The study was approved by the ethical committee of the Tehran University of Medical Sciences. All methods were performed in accordance with the relevant guidelines and regulations.
Not applicable.
The authors declare no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

Bakhtiari, A., Mostafavi, H., Mohamadi, E. et al. Identifying knowledge gaps in social determinants of health and related challenges in Iran; 2023. Health Res Policy Sys 23, 63 (2025). https://doi.org/10.1186/s12961-025-01300-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12961-025-01300-4