Reproductive Health volume 22, Article number: 119 (2025) Cite this article
Adolescent pregnancy remains a critical global health issue, with the World Health Organization reporting a prevalence of 10.3%. Pregnant adolescents aged 10 to 19 face elevated risks of mental health challenges, including depression, anxiety, and stress. Despite these vulnerabilities, there is a notable lack of effective psychosocial interventions, particularly in low- and middle-income countries. This study aims to develop and evaluate a culturally tailored psychosocial support intervention to improve mental health outcomes among pregnant adolescents in Iran.
This mixed-methods study comprises three sequential phases. First, a qualitative study will explore the experiences and perceptions of pregnant adolescents regarding psychosocial support. Second, insights from the qualitative phase will inform the development of a targeted intervention, guided by expert consensus using the Nominal Group Technique. Third, a quantitative phase will assess the intervention’s effectiveness through a randomized controlled trial involving 84 pregnant adolescents. Key outcomes will include levels of social support, anxiety, depression, and stress, measured using validated instruments. Data collection will involve semi-structured interviews, expert panels, and pre- and post-intervention assessments.
The study is expected to advance understanding of the psychosocial needs of pregnant adolescents and provide evidence for culturally sensitive interventions. The findings aim to inform clinical practice and health policy, contributing to improved mental health and overall well-being among this high-risk population.
This study has been approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1402.140) and registered with the Iranian Registry of Clinical Trials on June 26, 2023 (IRCT20190129042544N1).
The World Health Organization (WHO) identifies teenage pregnancy as a pressing global health concern, affecting countries across all income levels—high, middle, and low [1] Adolescent pregnancy is defined as pregnancy occurring in girls aged 10 to 19 years [2]. Currently, the global teenage pregnancy rate stands at 10.3% [3]. The highest numbers of adolescent births are reported in East Asia (95,153) and West Africa (70,423) [4], contributing to an estimated 15 million births annually among teenagers, approximately 11% of all births worldwide [5]. In Iran, which has a predominantly young population, the adolescent fertility rate has shown a fluctuating yet upward trend over the past decade. In 2010, the rate was approximately 33.36 births per 1,000 women aged 15–19, rising slightly to 33.96 in 2011. By 2020, this rate had increased significantly to 40.81 per 1,000, highlighting a growing trend in adolescent fertility [6]. Projections suggest a further increase by 2025, influenced by contributing factors such as early marriage and cultural norms that support childbirth shortly after marriage [7, 8].
Pregnancy during adolescence occurs at a pivotal developmental stage and poses significant risks to mental health. Adolescents undergoing this transition must simultaneously navigate the challenges of growing into adulthood, coping with an unplanned pregnancy, and assuming the responsibilities of early motherhood. These overlapping life changes can disrupt normative developmental trajectories and heighten susceptibility to both psychological and physical health disorders [7]. Research consistently shows that adolescent mothers experience higher levels of depression, anxiety, and stress compared to older pregnant women, a disparity potentially exacerbated by the biological and hormonal changes unique to this age group [9].
According to the Canadian Pediatric and Adolescent Gynecology and Obstetrics (CANPAGO) Committee, the prevalence of depression among adolescents ranges from 4 to 8%, but during pregnancy, this rate can rise sharply to between 16% and 44% [10]. These alarming figures underscore the need for targeted interventions to address the mental health challenges associated with adolescent pregnancy and childbirth.
Psychosocial support has emerged as a promising intervention strategy. As noted by Marzieh Bagheri Nia in her 2020 review, psychosocial support can reduce stress and improve mental health outcomes among pregnant adolescents, thereby enhancing their overall well-being [11]. Such interventions typically include the provision of information, emotional support, and counseling services that help adolescents build effective coping strategies. For example, a program implemented in Turkey that combined psychosocial support with educational sessions significantly reduced levels of anxiety and depression while enhancing perceived social support among pregnant adolescents [12]. Likewise, couple-focused counseling interventions have demonstrated effectiveness in reducing pregnancy-related anxiety in first-time adolescent mothers by actively involving their partners in the support process [13].
Despite encouraging findings, notable gaps and challenges persist in the current body of research. There remains a lack of robust evidence on the effectiveness of psychosocial interventions in preventing or managing mental health issues—such as depression, anxiety, substance use, and risky sexual behaviors—among pregnant adolescents. A significant limitation is the concentration of existing studies in high-income countries, underscoring a critical research deficit in low- and middle-income settings where such interventions are often most urgently needed [14]. Cultural and societal attitudes toward adolescent pregnancy and mental health significantly influence the support systems available to young mothers. In some societies, teenage pregnancy is heavily stigmatized and associated with shame, limiting access to psychological and social support. In contrast, other cultural contexts, particularly where early marriage is common, may normalize adolescent pregnancy, potentially reducing stigma but also overlooking the specific mental health needs of this group. These cultural dynamics emphasize the necessity for interventions that are not only evidence-based but also culturally sensitive and adaptable to different social contexts [12, 15]. This study seeks to address these gaps by developing and evaluating a psychosocial support intervention tailored to the unique needs of pregnant adolescents in Iran. The research adopts a mixed-methods approach, beginning with a qualitative exploration of adolescents’ experiences with psychological support during pregnancy. These insights, combined with expert input, will inform the design of a culturally relevant intervention. The intervention’s effectiveness will then be assessed through a quantitative study measuring key mental health outcomes. Findings from this research aim to enrich the existing knowledge base and offer practical guidance for healthcare providers and policymakers seeking to improve support systems for this vulnerable population.
To explain the perception and experience of pregnant adolescents from psychosocial support.
The choice of research method depends on the nature of the phenomenon under investigation and the specific research questions being addressed [16]. This study aimed to evaluate the effectiveness of a psychosocial support intervention on the mental health of pregnant adolescents. To accomplish this, a mixed-methods research design was employed, integrating qualitative and quantitative approaches across three phases.
In the first phase, a qualitative method was utilized to explore the lived experiences of pregnant adolescents who received psychosocial support, providing in-depth insights into their needs and challenges. In the second phase, the Nominal Group Technique was applied to prioritize and select intervention strategies based on both qualitative findings and expert consensus. Finally, the third phase employed a quantitative method to assess the impact of the developed intervention on key mental health outcomes, including social support, depression, anxiety, and stress.
Given the complexity of the research questions and the multifaceted nature of the intervention, a mixed-methods approach was deemed the most appropriate and comprehensive strategy for this study (See Fig. 1).
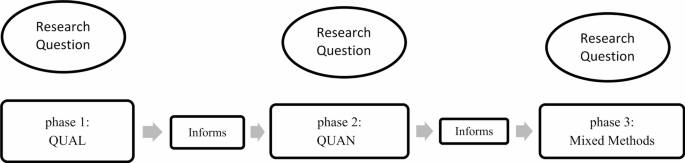
Mixed-methods design
The first phase of the study aimed to explore and understand the psychological support needs of pregnant adolescents. Participants were initially selected through purposive sampling based on their willingness to participate and ability to communicate effectively. As the study progressed, additional stakeholders including healthcare personnel, spouses, and family members of the adolescents were also recruited to provide broader perspectives on the adolescents’ psychosocial needs.
Interviews were conducted in health centers affiliated with Ahvaz Jundishapur University of Medical Sciences. The sample size was not predetermined; instead, sampling continued until data saturation was reached, ensuring the collection of rich and comprehensive qualitative data.
Qualitative stage: data collection method, sample size and, key participants selection
The primary method for data collection in the qualitative phase was semi-structured, in-depth interviews conducted with pregnant adolescents at health centers. Prior to the interviews, the researcher obtained written informed consent, coordinated with health center administrators, and provided participants with a clear explanation of the study’s purpose and procedures.
Purposeful sampling was employed to ensure diversity across various demographic and psychosocial factors. Face-to-face interviews were conducted using open-ended questions designed to explore experiences and perceptions of psychosocial support during pregnancy. The length of each interview varied depending on the participant’s condition and the depth of the topics discussed.
Examples of guiding questions included:
All interviews were audio-recorded with the participants’ permission, transcribed verbatim, and subjected to rigorous qualitative analysis. Ensuring the accuracy and integrity of the findings is a critical concern in qualitative research. To address this, the study adopted Lincoln and Guba’s [17] framework for evaluating trustworthiness, which includes credibility, dependability, transferability, and confirmability. In the later development of their constructivist paradigm, they also introduced authenticity as a fifth criterion to further validate the qualitative findings [18].
Ability to understand and speak Persian
Low-risk pregnancy and singleton pregnancy
Age 13–19
Willingness to participate in research
Ability to provide rich and adequate information in the subject matter of study
Being literate
The absence of any known mental-physical illness.
Participants were excluded from the study if they experienced any of the following:
In the second phase of the study, the psychosocial support intervention was designed through a structured, multi-step process. First, the key components and dimensions of the intervention were identified by integrating insights from the qualitative findings with a comprehensive review of existing literature and resources.
Next, intervention strategies were prioritized and refined using expert input obtained through the Nominal Group Technique, ensuring alignment with the psychosocial needs of the target population. This consensus-building process helped determine the most appropriate and feasible type of intervention.
Finally, the selected components were synthesized into a final version of the intervention, which was reviewed and validated by academic experts and professionals in the field prior to implementation.
The first part of this stage focused on identifying the key components of a psychosocial support intervention tailored for pregnant adolescents. This process drew upon findings from the qualitative phase, alongside an extensive review of both national and international literature. By synthesizing these two sources experiential data and evidence-based practices we aimed to ensure that the intervention design was contextually relevant and informed by global best practices.
To enhance the comprehensiveness of the intervention, literature from Iran and other countries was examined to integrate relevant insights, recommendations, and case examples. This culminated in the development of a preliminary version of the intervention.
Guided by the PICO framework, the central research question was defined as: “What types of interventions are implemented to improve psychosocial support for pregnant adolescents?”
A systematic search was conducted across multiple English and Persian language databases including ProQuest, Google Scholar, PubMed, SID, Iran Medex, Magiran, Scopus, and Web of Science without time limitations. The retrieved studies and resources provided a foundational basis for refining and constructing the initial draft of the intervention (See Tables 1 and 2).
In the second part of the intervention design phase, the Nominal Group Technique (NGT) was employed to prioritize and select the most appropriate psychosocial support strategies for pregnant adolescents. This structured, consensus-driven method brought together a multidisciplinary panel of experts, including professionals from health, education, and care services, to evaluate and refine the intervention components based on the findings from the qualitative phase.
The expert meeting focused on reviewing and prioritizing the needs and strategies previously identified. NGT is a practical and systematic approach that combines both qualitative discussion and quantitative scoring to facilitate decision-making. Its purpose in this context was to help set community-based healthcare priorities with a focus on maternal mental health.
Prior to the session, all panel members were provided with an overview of the study and a summary of the extracted qualitative findings. They were then asked to independently evaluate and prioritize the proposed components based on relevance, feasibility, and cultural appropriateness.
The expert panel comprised 10 professionals, selected for their academic qualifications and substantial experience in the field of maternal and adolescent mental health. The composition of the panel was as follows:
These experts contributed to the validation of the intervention content, offered guidance on cultural adaptation, and provided ongoing consultation throughout the intervention’s design and implementation phases. The diversity of professional backgrounds ensured a comprehensive evaluation of the intervention strategies from multiple perspectives [16].
The Nominal Group Technique (NGT) was conducted in a structured manner to ensure balanced participation and consensus among experts. The process included the following steps:
Discussion on the selected ideas
Although not an essential step in the formal NGT, a concluding discussion was conducted to help the group reflect on and integrate their final rankings [19]. Following the voting, priorities were ranked and presented to the group based on the established scoring criteria.
The intervention content was adjusted based on the prioritization of psychosocial support. This prioritization was derived from the results of the qualitative phase, the review of texts, and the Nominal Group discussions.
The third stage of the study will employ a randomized controlled clinical trial (RCT) design with two parallel groups to evaluate the effectiveness of a psychosocial support intervention compared to routine prenatal care among pregnant adolescents in Ahvaz, Iran.
A total of 84 pregnant adolescents will be recruited from health centers affiliated with Ahvaz Jundishapur University of Medical Sciences. Participants will be randomly assigned to either the intervention group, receiving psychosocial education, or the control group, receiving routine prenatal education as per existing healthcare protocols.
The intervention will be delivered through childbirth preparation classes, conducted in accordance with the national guidelines of the Iranian Ministry of Health, Treatment, and Medical Education. These classes will consist of eight sessions, each lasting two hours, and will be held between gestational weeks 20 to 37. Each session will include the following components:
Instructional methods may include videos, audio playback, music, posters, anatomical models (mannequins), whiteboards, and slide presentations, tailored to enhance learning and engagement [20]. This phase aims to quantitatively assess the impact of the psychosocial intervention on mental health outcomes, such as depression, anxiety, stress, and perceived social support, in comparison to routine care.
Prior to the implementation of the intervention, three structured workshop sessions will be conducted by the researcher for midwives and educators. These workshops are designed to build the participants’ capacity to deliver adolescent-centered psychosocial support, ensuring consistency and quality in the intervention delivery.
The workshop content will cover the following key areas:
The workshops will be led by the principal researcher, a Ph.D. candidate in midwifery with a Master’s degree in midwifery counseling. She has also completed university-level training in life skills education and communication skills.
All training sessions will be supervised by a senior academic advisor with a Ph.D. in counseling, who will oversee the content delivery to ensure both academic rigor and clinical relevance. This supervision will help maintain fidelity to the intervention model and reinforce best practices in psychosocial care.
Participant recruitment and consent
Eligible participants will be enrolled by the researcher based on predefined inclusion criteria. Following approval from the relevant ethics committee and research department, written informed consent will be obtained from all pregnant adolescents participating in the study.
Sampling and randomization
Participants will be recruited using an available (convenience) sampling method from selected health centers affiliated with Ahvaz Jundishapur University of Medical Sciences. A total of 84 adolescent pregnant women who meet the inclusion criteria will be selected.
To ensure unbiased group allocation, a block randomization method (block size = 6; 1:1 ratio) will be used to assign participants to either the intervention group or the control group. The random allocation sequence will be generated by an independent statistician using a random number table. Each participant will be assigned a specific code, and group allocation will be concealed in sealed, opaque, non-transparent envelopes. These envelopes, prepared in advance by individuals not involved in the intervention, will be stored securely at the health centers.
Group allocation procedure
At the time of enrollment, midwives at the health centers will open the sealed envelopes to determine each participant’s group assignment. This process ensures allocation concealment and randomization integrity throughout the trial.
The intervention will be conducted by midwives who have completed structured training workshops on adolescent-centered psychosocial support. The intervention will consist of 6 to 8 weekly sessions, each lasting 90 min, held in small groups of 5 to 7 participants.
Session content includes
Instructional methods
This structured approach is designed to empower pregnant adolescents with practical skills and emotional support to improve their psychosocial well-being throughout pregnancy.
Before the intervention begins, all pregnant adolescents in both the intervention and control groups will be asked to complete a series of questionnaires. These include a Demographic and Social Profile form, a Midwifery History questionnaire, the Vaux Social Support Scale, the Perceived Stress Scale, and the Depression, Anxiety. These tools have been selected to evaluate the participants’ psychological and social well-being at baseline.
Following the completion of the intervention sessions, the same set of questionnaires will be administered again, immediately after the final session, and once more four weeks later, to assess changes over time. The researcher will be responsible for distributing and collecting the questionnaires at each of these three time points, ensuring consistency throughout the study.
While it is not possible to blind either the researcher or the participants due to the nature of the intervention, steps will be taken to minimize bias. All data will be coded anonymously, and the questionnaire responses will be entered and analyzed by an individual who is not informed of the study’s objectives or group assignments.
To ensure the ethical integrity of the study, participants in the control group will receive a summary booklet containing the key content of the intervention sessions after data collection has been completed. Additionally, if any control group participants express interest in further support, they will be offered an individual counseling session following the intervention period.
All statistical analyses will be performed using SPSS software, version 26.0 (SPSS Inc., Chicago, IL, USA). A significance level of p < 0.05 will be used for all tests. To maintain the validity of the findings, an intention-to-treat (ITT) analysis will be applied. This approach ensures that all participants are analyzed in the groups to which they were originally assigned, regardless of whether they completed the intervention, thereby preserving the randomization process and increasing the reliability of the results.
The study population will include all adolescents referred to medical and health centers affiliated with Ahvaz University of Medical Sciences.
The research will be conducted in medical and health centers under the affiliation of Ahvaz University of Medical Sciences.
The study will focus on pregnant adolescents receiving care at the selected health centers affiliated with Ahvaz University of Medical Sciences.
Data from the quantitative part of the study will be collected through separate questionnaires.
Quantitative data will be collected using validated, self-administered questionnaires.
The following validated Persian versions will be used, all of which have demonstrated strong reliability and internal consistency in prior Iranian studies:
The primary outcome for sample size calculation is based on the effectiveness of an Early Depression Prevention Program for pregnant adolescents, as described in previous randomized controlled trials” [25]. According to these studies, 38 participants per group are required. Allowing for a 10% dropout rate, the final sample size is set at 42 per group, totaling 84 participants. The calculation was performed using MedCalc software, with a power of 90% and a significance level of 5%.
This structure ensures clarity and directly references the reliability and validation of the instruments used, as well as the rationale for sample size determination.
$$\:\text{z}\_\:(1-/2)\hspace{0.17em}=\hspace{0.17em}1.96$$
$$\:\text{z}\_\:(1-)\hspace{0.17em}=\hspace{0.17em}1.645$$
$$\:\text{S}\text{D}\_1\hspace{0.17em}=\hspace{0.17em}9.14$$
$$\:\text{S}\text{D}\_2\hspace{0.17em}=\hspace{0.17em}15.83$$
$$\mu\:\_1\hspace{0.17em}=\hspace{0.17em}73.47$$
$$\:\mu\_2\hspace{0.17em}=\hspace{0.17em}64.39$$
$$\mathbf{76}\boldsymbol=\mathbf2\frac{\mathbf{\left({1.96+1.645}\right)}^{\mathbf2}\boldsymbol+\mathbf{\left({9.14_1^2+15.83_2^2}\right)}}{\mathbf{\left({37.47-64.39}\right)^\wedge2}}$$
$$\:\mathbf{n}=2\frac{{\left({\mathbf{z}}_{1-\raisebox{1ex}{$\varvec{\upalpha\:}$}\!\left/\:\!\raisebox{-1ex}{$2$}\right.}+{\mathbf{z}}_{1-\varvec{\upbeta\:}}\right)}^{2}+{(\mathbf{S}\mathbf{D}}_{1}^{2}{+\mathbf{S}\mathbf{D}}_{2}^{2})}{({\varvec{\upmu\:}}_{1}-{\varvec{\upmu\:}}_{2})^\wedge2}$$
The initial sample size calculation determined that 38 adolescents were needed in each group, totaling 76 participants. To account for a potential 10% dropout rate, the adjusted sample size was increased to 42 adolescents per group, resulting in a total of 84 participants.
Statistical analysis for this study will be conducted using SPSS version 26.0, with a significance threshold set at P < 0.05. To begin, the normality of all quantitative data will be assessed using the Kolmogorov-Smirnov test. For comparisons between groups, independent t-tests will be employed for variables that are normally distributed, while the Mann-Whitney U test will be used for those that do not meet normality assumptions.
To evaluate changes within groups over time, repeated measures ANOVA will be applied to outcomes that are normally distributed. If the data violate the assumptions required for repeated measures ANOVA, such as normality or sphericity, non-parametric alternatives like the Friedman test will be used instead.
To control for potential confounding variables, Analysis of Covariance (ANCOVA) will be conducted. All statistical tests will be two-tailed, and results will be considered statistically significant at a P-value of less than 0.05.
Social support
Pregnancy anxiety
Pregnancy depression
Pregnancy stress
The integration of quantitative and qualitative data occurs during the analysis and interpretation phases (see Fig. 2). Data collection and analysis are conducted in two distinct stages to address different research questions.

Study diagram
The study begins with a qualitative approach and a literature review to explore and understand the experiences of psychosocial support among pregnant adolescents. Based on the qualitative findings, priorities are identified and an appropriate intervention is designed. Subsequently, a quantitative method is employed to evaluate the impact of the intervention on maternal outcomes.
In the final stage, the qualitative and quantitative data are combined for comprehensive analysis and interpretation. This mixed-methods integration enhances the validity and depth of the findings, providing a more complete understanding of the phenomenon and supporting the development of effective, context-specific solutions.
The first phase of the study has been completed. We are currently in the initial stage of the second phase, which involves conducting a comprehensive literature review (see Table 3).
Our evaluation categorizes interventions into three primary domains: school-based, community-based (including home and social environments), and health-based interventions. This framework is directly informed by our study’s findings, which highlighted distinct sources and types of support as reported by adolescents, families, and healthcare providers. Specifically, the qualitative data revealed that schools are key platforms for delivering reproductive health education and life skills (school-based interventions); families and community networks play a vital role in providing emotional and social support, including home-based care (community-based interventions); and healthcare centers are essential for offering adolescent-friendly reproductive and prenatal services (health-based interventions).
When planning care for pregnant adolescents, it is essential to address the multifaceted consequences of pregnancy by considering physical, psychological, and social dimensions.
This foundational tier emphasizes specialized care for pregnant adolescents, including the provision of comprehensive sexual and reproductive health information, youth-specific services, and improved access to prenatal, perinatal, and postnatal care [26]. According to the World Health Organization (WHO), adolescent-friendly health services should be accessible, acceptable, equitable, appropriate, and effective, addressing the unique developmental needs of adolescents [27]. Studies have shown that tailored, adolescent-specific programs can significantly increase prenatal care attendance and improve pregnancy outcomes, such as reducing rates of preterm birth and low birth weight [28]. Education on the risks of unsafe abortion is also critical, particularly in settings where adolescents face legal or social barriers to safe abortion services. Unsafe abortion remains a major contributor to maternal morbidity and mortality among adolescents, who often lack knowledge and access to safe procedures [29]. These recommendations align with the perspectives of study participants, who emphasized the need for medical and psychological care tailored to the unique developmental stage of adolescents. Implementing adolescent-friendly, culturally sensitive health services is a key step toward improving outcomes for this vulnerable population.
The second tier focuses on preventive measures, such as delaying early marriage, providing robust social [30] and psychological support [31, 32], implementing home-based care [33, 34], and offering life skills education aimed at self-care [35]. Engaging male partners and broader family networks in these initiatives is also critical for creating a supportive environment [36]. Evidence suggests that male involvement enhances maternal well-being, improves partner communication, and fosters shared responsibility in reproductive health [37]. These findings emerged from thematic analysis of interviews with families and adolescents, who highlighted the pivotal role of community, peer, and familial networks in shaping their pregnancy experiences.
At the systemic level, establishing specific laws and policies is imperative. This includes preventing early marriage, creating opportunities for continued education and employment, and ensuring adequate nutrition and healthcare access for pregnant adolescents, particularly in rural, marginalized, and low-income communities [11, 14, 38]. Our results underscore the importance of integrating psychosocial and reproductive health education into school curricula, as suggested by participants who identified schools as accessible and influential settings for early intervention.
Psychosocial support plays a vital role in delivering emotional, psychological, and social assistance, especially during challenging periods. Adolescent mothers require targeted psychosocial support throughout their pregnancies to enhance their emotional well-being, self-esteem, and resilience [39]. This support encompasses various interventions, including therapy, peer support, and educational programs focused on parenting and essential life skills [9].
Research indicates that interventions providing psychosocial support significantly benefit teenage mothers by promoting healthier behaviors, increasing the likelihood of seeking prenatal care, and developing effective coping strategies. Such support not only improves mental well-being but also enhances parenting capabilities and strengthens family relationships. Furthermore, adequate psychosocial support facilitates access to community resources, thereby establishing a robust support network for young mothers and their children [30, 31, 36, 40,41,42,43].
The general guidelines of the Ministry of Health and the educational programs of universities of medical sciences in Iran do not specifically address the psychological, social, or developmental needs of teenage mothers. However, Iranian studies consistently show that pregnancy during adolescence requires special attention. For example, one study demonstrated that group-based prenatal care (GPNC) significantly increases the empowerment of pregnant adolescent mothers; appropriate education and support through GPNC can improve mental health, self-esteem, and social interactions among these young women [44]. Despite this, current standard programs typically offer common content for all pregnant mothers, without a separate program or specific agenda for pregnant adolescents [20]. These findings underscore the need for a more tailored, holistic approach, one that addresses the distinctive psychosocial and developmental needs of pregnant adolescents, rather than relying solely on generalized maternal health programs.
Overall, while existing guidelines provide a foundation for prenatal care, a dedicated, adolescent-focused strategy is essential to ensure that the complex and multifaceted needs of this vulnerable group are adequately met.
This study presents several strengths. It is pioneering in its approach to delivering psychosocial support specifically tailored to pregnant adolescents, drawing on insights from adolescents, families, healthcare providers, and experts regarding the unique psychosocial needs of this group. By incorporating international research, the study offers a comprehensive understanding of the phenomenon. The use of a mixed-methods approach further enhances the reliability of the findings and supports the development of a holistic psychosocial support program within Iran’s health system.
The study aims to evaluate the effectiveness of psychosocial interventions on pregnancy outcomes among adolescents, with a focus on promoting positive mental health and addressing factors that may threaten the well-being of pregnant teenagers and young parents. While the findings may not be universally generalizable due to differences in healthcare systems and sociocultural contexts, they offer valuable insights that can be adapted to various settings.
However, there are some limitations to this study. The primary focus on mental health outcomes may inadvertently overlook important physical health aspects. Additionally, including teenagers in pregnancy classes alongside adults may not be the most effective pedagogical approach, and there may be insufficient infrastructure to adequately train all pregnancy class instructors.
Despite these limitations, the findings of this study can serve as a foundation for planning effective interventions to promote mental health among pregnant adolescents. These results are accessible to stakeholders and healthcare providers working with this population. Insights from this research can be integrated into childbirth preparation classes and midwifery education, providing valuable guidance for future research and the development of tailored support programs for pregnant adolescents, particularly in low- and middle-income countries.
This study focused on the development, implementation, and comprehensive evaluation of a culturally appropriate psychosocial intervention to promote mental well-being among pregnant adolescents in Iran. Through a comprehensive, multi-phase approach, including qualitative exploration, expert validation using the Nominal Group Technique, and a randomized controlled trial, the research directly addresses the urgent mental health needs of this vulnerable group. The intervention is firmly grounded in evidence and prioritizes psychological empowerment, stress management, and the reduction of depression and anxiety, while also strengthening social support networks for pregnant adolescents. These elements are crucial for fostering resilience and promoting overall well-being during adolescent pregnancy.
A key strength of this study is the involvement of trained midwives in delivering the intervention, ensuring both its practicality and its potential for seamless integration into existing maternal care services. Should the intervention prove effective, it could serve as a model for the development of adolescent-focused mental health programs within reproductive healthcare systems, influencing both national policy and global health strategies. Moreover, the insights gained from this research may be applicable to other low- and middle-income countries facing similar challenges, thereby advancing the global agenda for adolescent maternal mental health.
No datasets were generated or analysed during the current study.
- WHO:
-
World Health Organization
- NGO:
-
Non-governmental organization
- CANPAGO:
-
Canadian Pediatric and Adolescent Gynecology and Obstetrics (CANPAGO) Committee
- UNICEF:
-
United Nations Children’s Fund
- MDGs:
-
Millennium Development Goals
- QUAL:
-
Qualitative
- QUAN:
-
Quantitative
- NGT:
-
Nominal Group Technique
- EDS:
-
Edinburgh Depression Scale
The study is part of the results of the PhD dissertation of the first author in midwifery (research project number: 330101729). The authors would like to thank all the participants in this study and Ahvaz Jundishapur University of Medical Sciences in Iran. We want to thank Mr. Navid Jahanshahi, PhD Candidate at the Faculty of Letters, University of Lisbon, and member of the Lisbon Baby Lab, for his assistance in editing the English language of this manuscript.
The current review’s findings can support experts and healthcare providers in developing effective interventions to reduce teenage pregnancy complications.
The present study was conducted with financial support from the Office of Research and Technology at Jundishapur Ahvaz University of Medical Sciences, under Grant Number 330101729.
This study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Science (IR.AJUMS.REC.1402.140). The study will conduct in accordance with the Declaration of Helsinki. Additionally, the study protocol was registered in the Iranian Registry for Randomized Controlled Trials 2023-06-26 (IRCT20190129042544N1).
We will ask for permission from all the participants before including them in the study. We will draft a comprehensive consent form for all research participants. The form will contain a clear and concise explanation of the research, and participants will be required to read, complete, and sign the form. In addition to obtaining permission to record interviews, measures will be implemented to ensure the confidentiality of all information and the anonymity of individuals involved in the study and its findings.
Not applicable.
The authors declare no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

Cite this article
Yousefi, S., Montazeri, S., Javadifar, N. et al. Design, implementation, and evaluation of a psychosocial intervention to improve mental health in pregnant adolescents: a mixed-methods protocol. Reprod Health 22, 119 (2025). https://doi.org/10.1186/s12978-025-02060-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-025-02060-8










